|
Autism Spectrum Disorder and Substance Use Disorders Lisa R. Macafee May 24, 2022  This paper discusses the unique challenges that individuals on the autism spectrum face with substance abuse disorders. To honor autism advocacy groups, individuals with autism will be referred to mostly using identity-first language of “autistic” as opposed to person first language of “a person with autism” and for this paper, autistic includes all diagnosis that were previously under the autism spectrum disorder umbrella in the DSM-IV. While many disabilities are separate from the core of an individual, autism is a difference in neurology, so many autistic people experience autism as part of what shapes their core. I am a 40-year-old autistic person who received my diagnosis at age 37 after being in and out of therapy for autism-related symptoms and traumas and struggled with substance use when I was younger. I wanted to explore the variety of reasons autistic individuals turn to substance use and what therapies and treatments are most effective for this population.
Autism and substance Abuse Autism is a developmental disorder that includes deficits in social reciprocity, social communication, and restricted, uncompromising, or rigid interests and activities (Helverschou, Brunvold, Arnevik, 2019). Autism in adults is a field with underdeveloped research because only recently have adults been diagnosed with autism, and clinical diagnosis are still more commonly understood to be diagnosed as children, and with a bias towards male children. High functioning autistic people often go undiagnosed in childhood, and without treatment in adulthood, may find other ways to manage their symptoms such as substance abuse. 44% of autistic clients took more than two years in psychiatric care to receive an autism diagnosis, and it is estimated that many adult autistics are undiagnosed and underserved, leading to increased co-morbid disorders that could have been preventable (Nylander, et al., 2013). Diagnosis of autism is on the rise in the last 20 years. Many attribute the increase in diagnosis to broadened diagnostic criteria and increased awareness about atypical and high-functioning autism presentation. While no one knows the cause of autism, certain factors can lead to higher prevalence. One such factor is opioid use of the mother during pregnancy (Feder, 2020). Other contributing factors include heavy drinking, smoking cigarettes, or being exposed to neurotoxic chemical pollutants such as lead and mercury during pregnancy. Autism is also highly hereditary, leading some to ask if autism is caused by substance use of the parent, or if the parent use substances because of their (un)diagnosed autism, and the autism is simply genetic? It seems that autism is about 20% - 30% genetically predictable and environmental factors affect the neuropsychiatric development of an individual with genetic susceptibility for autism (Xi, Wu, 2021). Approximately 0.6% of the global population struggles with substance use disorder (SUD), and individuals with conditions such as personality or affective disorders, anxiety, schizophrenia, bi-polar disorder, PTSD, and attention deficit hyperactivity disorder (ADHD) are affected by SUD more than others (Helverschou, Brunvold, Arnevik, 2019). Lifetime rates for substance-use disorder (SUD) globally range from between 10% to 20% (Kronenberg, et al., 2015). Autistic individuals struggle with substance abuse at close to a doubled rate than their neurotypical peers with 19-30% of autistic clients in clinical settings also struggling with substance abuse. While many autistic adults have negative attitudes towards psychoactive substances, possibly due to most being illegal, interestingly, the more autistic traits a person exhibits, the higher their risk of substance-use disorder. It is also true that 1st degree relatives of an autistic person have a higher risk of substance-use disorder. This suggests that there may be genetic, shared environmental, or epigenetic factors surrounding autism that lend towards substance use (Butwicka, et al., 2017). Between 1% - 2% of the population is autistic and autistic individuals are at risk for many secondary problems, including substance abuse. Autistic people are up to seven times more likely to come into contact with the criminal justice system than their neurotypical peers, and the autism community has generally responded with dissatisfaction or even been traumatized from their treatment by police. Police may in part respond to autistic individuals negatively because some autistic traits can be confused for signs of substance use or aggression including avoiding eye contact, egocentricity, social communication impairments, and dependence on routines. Police can easily perceive a struggle to verbally respond appropriately under stress as deliberately ignoring or refusing to comply. This difficulty in responding appropriately to the police is of course exacerbated by substance use of an autistic person. Autistic people tend to respond most positively when approached quietly, calmly, in a non-threatening manner (Mogavero, 2018). There are many reasons that substance use may appeal to autistic people. At the top of the list are decreased social anxiety and increased (self-perceived) social functioning and reducing overall tension (Butwicka, et al., 2017). I will say that for myself, I turned to substance use because it was the only time I felt part of a social group. If everyone was intoxicated, they were all unable to make correct social interactions and my inability to predict subtle social cues was mitigated by no one expecting complex social interactions when high or drunk. It seemed to me that when other people were high or drunk seemed to be the time I had the easiest access to meaningful conversations and social interactions. When sober, I found it difficult to engage with people and became much more reserved. It took years of therapy for me to be able to comfortably interact with individuals socially sober, and even now, in new situations or with people I don’t know, I find it challenging. Overall, individuals with autism report dissatisfaction with parts of their life that substance abuse can diminish or dull temporarily and those autistic individuals with SUD often receive ineffective care and treatment (Kronenberg, et al., 2015). While autistic individuals who are less socially proficient may be protected from peer influences of drugs or alcohol, autistic people who are socially outgoing and with higher intelligence have higher risk of substance use disorder. Screening for SUD during autism assessments is not standard procedure and it is likely that many high-functioning autistic people are missed for SUD upon assessment because they do not feel substance abuse pertinent to bring up when being supported for autism. Reasons for using substances as stated by 18 college students with ASD ranged from reducing social anxiety and inhibitions to finding peace, calming down, overcoming frustrations, or forgetting problems. Substance use is problematic when relied on long-term however, because of its effect to reduce already impaired social functioning. While getting drunk or high may reduce social anxiety temporarily, it also reduces the ability of the autistic person to judge what behaviors are socially acceptable in the setting they are in and they may experience consequences for unintentionally violating unspoken social mores and face increased social isolation or relationships challenges as a result of substance use after the fact (Helverschou, Brunvold, Arnevik, 2019). Assessment and treatment of primary, secondary, and co-morbid disordersDiagnosing autism and substance use disorder can be challenging because some autistic traits could be products of substance use (Helverschou, Brunvold, Arnevik, 2019). Also difficult to navigate in substance abuse treatment is that 55% of people seeking SUD treatment also have a co-occurring psychiatric disorder. Individuals with co-occurring disorders typically have more severe symptoms, higher relapse rates, higher risks of hospitalization and incarceration, serious infections, and unstable housing, which all contribute to greater treatment needs (Kronenberg, et al., 2015). Additional comorbid conditions complicate the rate of substance-use disorder among autistics as well. For example, autistic people who also have ADHD are more likely to have substance use disorder, while autistic people with intellectual disability are less likely to turn to substance use (Butwicka, et al., 2017). Approximately 60% of autistic individuals have co-occurring psychological disorders (Nylander, et al., 2013). The challenge for mental health providers of individuals with autism who also have SUD is that 87% of adult autistics also have a co-occurring mental illness, and often multiple diagnosis. Each symptom needs to be addressed for effective care, and this can get overwhelming for the client and the practitioner (Houting, 2019). Autism in general is likely underdiagnosed in adults who missed a diagnostic window as a child in k-12 education due to their presentation being milder. There is also a likelihood that females with autism are underdiagnosed due to diagnostic bias for males and higher masking social difficulties in females with autism. Autistic adults who are undiagnosed with autism are at a higher risk for mental health disorders, and possibly SUD due to untreated autism. Adults with autism have high rates of co-occurring disorders including intellectual disability, affective disorders, anxiety, and psychotic disorders, all applicable disorders will need to be taken into account for each individual to receive effective and individualized care (Nylander, et al., 2018). Adults who go undiagnosed often face increasing mental health problems as they cannot find the solution to why they cannot fit in, cannot understand what others imply is simple, and cannot navigate complex employment. Undiagnosed autistics often default to the idea that they are simply bad, and there may be a lot of work to do in therapy to address and reverse these ideas (Stagg and Belcher. (2019). It may be beneficial to screen for autism for clients with serious mental health disorders such as borderline personality disorder (BPD) as there are an often an overrepresentation of autistic traits present in clients with BPD and treating the autism symptoms separately, such as rigidity, patient-therapist communication issues, emotional understanding, executive function deficits, and difficulties relearning may be helpful for best outcome potential (Kaltenegger, Philips, Wennberg, 2020). One assessment tool that is free and available to the public online is the Autism-spectrum Quotient (AQ), which has been demonstrated to be effective in discerning if an individual may have enough autistic traits to warrant further exploration of a diagnosis. This assessment relies on self-reporting, so is not as reliable as a clinical assessment. For many in the possibly-autistic-and-exploring-options community, having a free and easy to access assessment to let them know they may be on the right track in even attempting to look into autism can be a lifeline. The AQ can also be used by practitioners who are less familiar with autism to determine to they should refer to a developmental psychologist or autism specialist for further testing. That being said, caution should be used when using assessments like these because many traits highlighted as autistic in the AQ could also be traits for obsessive compulsive disorder, social anxiety disorder, or ADHD (Sizoo, et al., 2009). While ADHD has been shown to have high rates of substance abuse disorder comorbidity and autism has not shown as high rates, autism often co-occurs with ADHD. About 28%-80% of autistic individuals also meet the diagnostic criteria or show signs of ADHD, but often will get one diagnosis or the other, and the 4th edition of the Diagnostic and Statistical Manual of Mental Disorders specifically prohibited an ADHD diagnosis in addition to an autism diagnosis, therefore it is likely that many autistic individuals are underdiagnosed for ADHD and at higher risk for SUD as well. Autistic individuals with SUD are more likely to abuse alcohol than illegal drugs because of the complex social interactions needed to secure illegal substances and the challenges that autism poses in negotiating these spaces (Kronenberg, et al., 2015). Recovery and resilience interventions for autistic substance abusers There have been few research studies to find appropriate SUD treatments for autistic individuals, and traditional processes such as group therapy may be counterproductive for some autistic clients because it may create undue stress in trying to verbalize substance abuse challenges while balancing social skills deficits. On a positive note, autistic clients may have higher levels of program completion once they decide they will enter treatment and may have greater potential for improvement because they were operating from a greater initial social deficit and theory of mind and mentalizing skills can be learned (Kaltenegger, Philips, Wennberg, 2020). 50% of clients drop out of SUD treatments before completing their programs, and autistic clients are more in need of individualized treatments. This is partly due to the fact that autistic folks with SUD tend to have more extensive and severe needs than their neurotypical peers, often involving not only medical, psychological, and social support, but also housing, transportation, education, and legal support (Helverschou, Brunvold, Arnevik, 2019). Autistic women often have increased needs than autistic men as they have increased risks of mortality, incarceration, and co-morbidity. There is a need for more research in this subgroup and how best to serve them (Olsson, Fridell, 2018). As clinicians working with SUD in the disability community may be working with a triple or more diagnosis and the client needs can be very intense, it is especially important to work collaboratively with other professionals. Collaboration with psychiatrists can be especially important to provide appropriate pharmaceutical interventions and ensure proper care and support around those pharmaceutical interventions. Often times, treatments should be prioritized and the clients understanding of what each treatment is for should be scaffolded so they are able to understand and be an active participant in their treatment path (Lakhan, 2020). One treatment method that shows promise for autistic individuals with SUD is adapted Cognitive behavioral therapy (CBT). Adaptations in CBT for autistic people include using familiar routines and activities with structured roles between the client and therapist to maintain predictability and structure that can help reduce anxiety. Similar to working in other sensitive groups, it can be helpful to set-up community guidelines for behavior of both client and therapist during treatment and set goals for treatment and decide on the treatment plan together. (Helverschou, Brunvold, Arnevik, 2019). I have used CBT for myself and autistic students and have found that it feels more tangible as a therapy option. CBT appeals to my autistic brain to have concrete tasks and explanations why this may work and seems to have more clear response goals, which I found helpful to have. Relapse prevention for autistic individuals and substance abuse To prevent relapse with autistic clients, therapy needs may need to be more extended than for a typical individual in substance abuse treatment. Therapists treating autistic people with SUD have said the therapy was more demanding than work with neurotypical SUD clients; they needed to be more structured, use more directive therapy strategies, and SUD treatment took more sessions. Treatment needs are partially so much more demanding because many autistic clients needed education about autism itself to understand how and why their brains operate differently than those around them, education about drugs to truly understand the scientific results of specific drugs on the brain and body, assistance navigating their social contacts and pro-social coping mechanisms to use when experiencing stress, housing assistance, leisure activities support and facilitation advice, and employment support to be able to function in their professional environment without relying on substance use to self-medicate. Some autistic clients tended to view their therapists as their friend and there was a higher-than-average emotional involvement with autistic clients that suggests a need for supervision and collaboration when working with autistic people in recovery (Helverschou, Brunvold, Arnevik, 2019). It is helpful for autistic clients with substance abuse disorder to be treated with integrated mental health support and substance abuse treatment instead of a fragmented separate care for each disorder. Finding a practitioner who can work with other specialists, autism experts, and psychiatrists and collaborate on appropriate care is essential for autistic people to receive effective support (Kronenberg, et al., 2015). Many autistic people have psychological care needs that bleed into physical care needs and care is most effective when all parties are operating with the same information. For example, I once became very sick with serotonin syndrome because I was on an anti-depressant and took two triptan migraine pills, not realizing these prescriptions could have a drug interaction. Clients need to be part of their therapies and feel included to prevent relapse. Treatment for autistic individuals with SUD should focus on helping the client learn coping and socialization skills so they can live their life to the fullest potential and reduce their troubling symptoms, so they are better able to function. Because autism affects so many areas of life that are also impacted by substance abuse, but the added issue of social impairment means that autistics often turn to substance use to help their social functioning, but substance use can have much more dramatic effects on an autistic individual because they cannot process their social interactions with the fluency of a neurotypical person, often resulting in significant support needs in mental health, financial literacy, unemployment, family and social interactions, adult living skills such as maintaining a home, activities, and sexual health support (Kronenberg, et al., 2015). Another component to consider for autistic people with deficits in social-emotional reciprocity and communication is that motivators that seem clear to the average person may not be clear to an autistic person and they may need potential harms explained to them. For example, an autistic youth caught for drug dealing did not immediately understand the harm that using drugs could have on minors because they did not have the ability for easy empathy and needed to have the effects described to them before they grasped the problem. For true rehabilitation, extinction of substance use, and social integration, explicit teaching of theory of mind and mentalizing skills is necessary (Riolo, et al., 2021). I believe that the most important components of effective care for an autistic person with substance abuse disorder are education about the exact and real functions of substance use on the brain and body, physical care support that may include prescriptions for anxiety and/or depression, which are rampant among adult autistics of normal intelligence, and especially common among adults autistic people with substance use disorder, emotional support in self-regulation and assistance in understanding social roles, expectations, and support to understand and meet these expectations, and traditional therapy of some sort to help the individual process through their experiences and find a way to feel grounded and to live a life of purpose. My biggest problems came from not knowing I was autistic and being desperate to “be normal” and not feel the constant anxiety of hypervigilance that was my life then. Help autistic people live their lives and help them find the meaning in their lives that allows for them to enjoy the process. References Butwicka, A., Långström, N., Larsson, H., Lundström, S., Serlachius, E., Almqvist, C., Frisén, L., & Lichtenstein, P. (2017). Increased Risk for Substance Use-Related Problems in Autism Spectrum Disorders: A Population-Based Cohort Study. Journal of Autism & Developmental Disorders, 47(1), 80–89. https://doi-org.csu.idm.oclc.org/10.1007/s10803-016-2914-2 Feder, R. (2020). Ten Years of Experience With Buprenorphine in a Private Psychiatric Outpatient Practice. American Journal on Addictions, 29(6), 508–514. https://doi-org.csu.idm.oclc.org/10.1111/ajad.13060 Helverschou, S. B., Brunvold, A. R., & Arnevik, E. A. (2019). Treating patients with co-occurring autism spectrum disorder and substance use disorder: A clinical explorative study. Substance Abuse: Research and Treatment, 13 Doi: HTTPs://doi-org.csu.idm.oclc.org/10.1177/1178221819843291 Houting, J. D., (2019, September). Why everything you know about autism is wrong. [Video file]. Retrieved from: https://www.ted.com/talks/jac_den_houting_why_everything_you_know _about_autism_is_wrong Kaltenegger, H. C., Philips, B., & Wennberg, P. (2020). Autistic traits in mentalization‐based treatment for concurrent borderline personality disorder and substance use disorder: Secondary analyses of a randomized controlled feasibility study. Scandinavian Journal of Psychology, 61(3), 416–422. https://doi-org.csu.idm.oclc.org/10.1111/sjop.12595 Kronenberg, L. M., Goossens, P. J. J., Etten, D. M., Achterberg, T., & Brink, W. (2015). Need for Care and Life Satisfaction in Adult Substance Use Disorder Patients With and Without Attention Deficit Hyperactivity Disorder (ADHD) or Autism Spectrum Disorder (ASD). Perspectives in Psychiatric Care, 51(1), 4–15. https://doi-org.csu.idm.oclc.org/10.1111/ppc.12056 Lakhan, R. (2020). Dual diagnosis in substance abuse assessment and treatment for alcohol and drug educators. Journal of Alcohol and Drug Education, 64(3), 84-86. Retrieved from http://proxy1.calsouthern.edu/login?url=https://www-proquest-com.csu.idm.oclc.org/scholarly-journals/dual-diagnosis-substance-abuse-assessment/docview/2507264742/se-2?accountid=35183 Mogavero, M. C. (2018). What do criminal justice students know about autism? an exploratory study among future professionals. Journal of Police and Criminal Psychology, 1-11. Doi: HTTPs://doi-org.csu.idm.oclc.org/10.1007/s11896-018-9302-0 Nylander, L., Axmon, A., Björne, P., Ahlström, G., & Gillberg, C. (2018). Older adults with autism spectrum disorders in Sweden: A register study of diagnoses, psychiatric care utilization and psychotropic medication of 601 individuals. Journal of Autism and Developmental Disorders, 48(9), 3076-3085. Doi: HTTPs://doi-org.csu.idm.oclc.org/10.1007/s10803-018-3567-0 Nylander, L., Holmqvist, M., Gustafson, L., & Gillberg, C. (2013). Attention-deficit/hyperactivity disorder (ADHD) and autism spectrum disorder (ASD) in adult psychiatry. A 20-year register study. Nordic Journal of Psychiatry, 67(5), 344–350. https://doi-org.csu.idm.oclc.org/10.3109/08039488.2012.748824 Olsson, T. M., & Fridell, M. (2018). The five-year costs and benefits of extended psychological and psychiatric assessment versus standard intake interview for women with comorbid substance use disorders treated in compulsory care in Sweden. BMC Health Services Research, 18 Doi: HTTPs://doi-org.csu.idm.oclc.org/10.1186/s12913-018-2854-y Riolo, A., Keller, R., Battaglia, R., & Albert, U. (2021). Probation of the offender with high functioning autistic traits and comorbidity. A case study. European Psychiatry, 64, S377. Doi: HTTPs://doi-org.csu.idm.oclc.org/10.1192/j.eurpsy.2021.1010 Sizoo, B. B., van den Brink, W., Gorissen-van Eenige, M., Koeter, M. W., van Wijngaarden-Cremers, P. J. M., & van der Gaag, R. J. (2009). Using the Autism-Spectrum Quotient to Discriminate Autism Spectrum Disorder from ADHD in Adult Patients With and Without Comorbid Substance Use Disorder. Journal of Autism & Developmental Disorders, 39(9), 1291–1297. https://doi-org.csu.idm.oclc.org/10.1007/s10803-009-0743-2 Stagg and Belcher. (2019). Living with autism without knowing: receiving a diagnosis in later life. Health Psychology and Behavioral Medicine. DOI: https://doi.org/10.1080/21642850.2019.1684920 Xi, T., & Wu, J. (2021). A review on the mechanism between different factors and the occurrence of autism and ADHD. Psychology Research and Behavior Management, 14, 393-403. Doi: HTTPs://doi-org.csu.idm.oclc.org/10.2147/PRBM.S304450
0 Comments
1/14/2022 AUTISTIC BEHAVIORS and developmental, physiological, psychological, and sociological causes and treatmentsRead Now Autistic Behaviors and Developmental, Physiological, Psychological, and Sociological Causes and Treatments
by Lisa R. Macafee Department of Psychology, California Southern University PSY 8701 Physiological Psychology Dr. Lucas January 15, 2022 Behaviors of autism While not strictly a behavioral disorder, most challenges for individuals with autism stem from managing the behaviors associated with having autism spectrum disorder (ASD). In this paper, ASD will be referred to interchangeably as autism, neurodivergent, or ASD. Individuals with ASD will be mostly referred to as autistic in this paper instead of the person-first language of ‘person-with-autism’ more commonly used in other disability rights movement. The autistic disability rights movement generally supports identity-first language because being autistic is core to our neurology and what makes us who we are, autism is not an accessory to who we are, it is an integral part of who we are. I am diagnosed autistic and will incorporate my own experiences, and those of my two autistic children into this paper. To be diagnosed as autistic according to the DSM-V, an individual needs to have, from an early age, significant deficits in social communication and two of the following behaviors: stereotyped or repetitive behaviors, inflexibility or insistence on routines, restricted or fixated interests (called by the autistic community “special interests”), or hyper or hypo-reactivity to sensory stimulus (CDC.gov, 2002). Core symptoms associated with autism are challenges in social communication, theory-of-mind, emotional control, cognitive function, executive function, perception, and motor control (Nabetani, Mukai, 2022). This paper will focus on the behaviors associated with an autism diagnosis and the developmental, physiological, psychological, and sociological causes, along with traditional and alternative treatments. Developmental causes Autism is defined as a developmental disorder. Pre-dispositions for autism are present from birth and become more apparent as individuals develop. Approximately 2% of the population has been diagnosed autistic and diagnosis are growing in rate due to broadened diagnostic criteria and increased awareness of differing ways autism can present. Males are still diagnosed three to four times as often as females, but this gap is shrinking as providers are learning how autism in girls looks different, and autistic girls tend to present with more social aptitude (Weir, Allison, Ong, Baron-Cohen, 2021). There may be a developmental factor involved in autism in where adaptive autistic traits are inherited independently, but when a threshold is crossed, these traits begin to synergize and reinforce cognitive development and neural connectivity in ways that can be socially maladaptive (Paul, Arora, Midha, Vu, Roy, Belmonte, 2021). Research demonstrates that higher prenatal androgen exposure correlates with decreased social functioning ability. This hypothesis explains why there are more males diagnosed with autism than females at a rate of four to one. This ‘extreme male brain theory’ posits that prenatal exposure to testosterone at critical developmental phases leads to autism. One metric used to assess prenatal androgen exposure is to measure the digit ratio of the index and ring fingers. Individuals exposed to more androgen in the womb typically have longer ring fingers and are typically male, but women with autism often have longer ring fingers as well. Other measurements of prenatal androgen include measurements of masculine traits in facial structure and umbilical cord testosterone levels. Each metric of androgen exposure leading to higher masculine traits correlates with higher autistic traits. Androgynous traits have also been correlated with higher rates of autistic traits as autistic females have more masculine faces, but autistic males have less masculine faces than their typical peers. I am an autistic woman whose ring finger happens to be longer than my index finger. I also have other masculine physical traits such as broad shoulders, and more masculine personality traits. This research fascinates me because my friends in school always described me as like a boy with ovaries, and I have to agree! Getting an autism diagnosis for myself explained so many of the questions I have had about why I was different from typical girls (McKenna, Huang, Vervier, Hofammann, Cafferata, Al-Momani,... Michaelson, 2021). Physiological causes One of the reasons autistic people tend toward routines is that our brains are wired for rule-based systematizing. While all people have some degree of autistic traits, the threshold for a diagnosis requires that these traits cause significant difficulty in life, and heightened levels of autistic traits scale with heightened levels of brain efficiency. Apparently, the brains of people with impaired social responsiveness and attention orienting show a greater efficiency of brain-wide functional networks and systematizing in the medial/anterior temporal lobe. In addition, individuals with higher traits of systematizing and difficulty in social perspective-taking (theory-of-mind) have brains with greater structural network efficiencies, mainly in the right temporoparietal junction. This greater brain efficiency could mean that autistic minds have specialized to have greater cognitive efficiency in non-social tasks. For example, I can research autism for hours, but have genuine anxiety about making a phone call and need to script out what to say. Autistic brains also seem to tend towards higher bottom-up gamma mediated connectivity and reduced top-down beta mediated signaling to information flow which could underlay these autistic brain differences (Paul, Arora, Midha, Vu, Roy, Belmonte, 2021). Autistic individuals tend to have restricted diets and have increased rates of eating disorders that can range from picky eating, anorexia, restricted food intake disorder, or bulimia. Autistic females are particularly more likely to engage in emotional eating behaviors and autistic individuals are overrepresented in having food allergies and sensitivities. Exercise is also challenging for some autistic individuals who may prefer screen time, aren’t as drawn by social motivation for team sports, or have motor control challenges that make playing sports less attractive. Sleep disturbances are common in autistic youth and adults and is not explained by epilepsy or other seizure disorders. These factors may explain why autistic individuals have increased rates of obesity and are at greater risk for chronic conditions such as type II diabetes, certain cancers, respiratory conditions, and cardiovascular conditions than their typical peers. Statistically, autistic individuals tend to have lifespans 16-38.5 years shorter than typical expectations. The importance of healthy diet, exercise, and sleep is underrated in much of the United States but seems particularly challenging to achieve for autistic individuals (Weir, Allison, Ong, Baron-Cohen, 2021). Psychological causes While autism is a developmental disorder and is part of the neurology of each individual, how each person is impacted by having autism varies dramatically. At times, peer interactions can create cyclical patterns that entrench the autistic individual in more autistic behaviors. For example, autistic individuals often experience social anxiety because they know they are different and want to have friends, but experience challenges in realizing these relationships. Negative peer experiences are associated with behaviors that autistic individuals experience when under stress, as will often be the case in social settings. For example, meltdowns are often experienced when the autistic individual cannot process more information and is being asked to engage with their environment more quickly than they are able to. When executive function starts to shut down after decision fatigue or masking, many autistic individuals find it difficult to keep up with hygiene demands or simply forget to wear deodorant or change clothes. As stressors mount, individuals may resort to rigid rule-keeping to maintain control over their situation. Self-injury may occur when the world is too “loud”, there are too many stimuli, and too many things happening at once. The difficult part of this is that the more negative peer interactions an individual experiences, the more likely they are to be stressed by social interactions, and the more likely they are to exhibit behaviors that lead to negative peer interactions! It’s a frustrating cycle for many individuals. It’s important to give autistic individuals tools to cope with their stressors that are more socially acceptable, such as finding socially appropriate stims (self-soothing or self-stimulating behaviors that allow the individual to manage stress) or finding ways to avoid having meltdowns in front of their peers (giving them a safe place to go and permission from teachers or supervisors to do so). Establishing routines that incorporate hygiene demands for the day help to both manage executive function stress by having less decisions to make and ensure hygiene is followed while hopefully leaving cognitive space for flexibility with peers, if their executive function is not overtaxed (Adams, Taylor, Bishop, 2020). Social anxiety disorder occurs at an alarming rate of 50%-70% in autistic adults and social anxiety rates correlate with social skills deficits. Social anxiety results in intense fear of, and negative evaluation of social situations and social situation avoidance. Experiencing difficulties with social interaction makes social interaction more anxiety-producing! This can be a self-reinforcing cycle as avoiding social situations leads to less competence in social situations, more anxiety, and poorer performance, which results in more social anxiety. Negative social experiences resulting from autistic behaviors increases bullying and rejection rates, while overstimulation from the senses can cause avoidant behaviors and anxiety to social situations as well. Experiencing social anxiety can lead to more intense behaviors associated with autism and more stress (Bemmer, Boulton, Thomas, Larke, Lah, Hickie, Guastella, 2021). If stressors are not appropriately managed, it becomes far too common for autistic individuals to experience depression and suicidal ideology. Having an autism diagnosis is often a protective factor against suicide. Those most at risk for suicidal thoughts and attempts are adults with a late diagnosis or no diagnosis. From my own experience of being diagnosed autistic at the age of 37, having that diagnosis was such a relief. It explained many of the challenges I experienced and allowed me access to others like me who have found coping strategies for the things we often struggle with. After receiving my own diagnosis, I went back to school to work in a career field that I enjoy, instead of continuing to work in a self-punishing environment. I allowed myself grace to care for myself and an autism diagnosis allowed me to look at myself as different instead of broken. Women are particularly underdiagnosed as autistic, and this has a harmful effect on their health as 40.6% of all people who attempted suicide without an autism diagnosis scored above the autism diagnosis cut-off and 45% or women who meet autism diagnostic criteria but are undiagnosed have made a suicide plan. 16% of these women attempted suicide. 11% of people with depression and 15% of women with borderline personality disorder also meet diagnostic criteria for autism and those with comorbid diagnosis are the individuals most at risk for suicide. I struggled with depression and anxiety when I was younger and wish I had learned more about autism because now I know that most of the pain and trauma I experienced was from now knowing why I was different. If I had a developmental and neurological fact (an autism diagnosis) to explain this difference, it would have made a great impact on the challenges I experienced (Cassidy, Bradley, Cogger-Ward, Rodgers, 2021). Sociological causes Autism is in no small part influenced by society around us. I have an autistic friend that states with firm belief that they are not internally disabled, only disabled by the way society expects us to react to it. While it is true that autistic individuals experience social communication and behavior challenges, we are often extremely efficient (I will get my projects done for work even if I’m working for free), trustworthy (I will not lie or betray what I believe is correct, but don’t ask me to lie for you!), reliable (I have called work from the ER to make sure they are doing okay without me and offer to send emails from the hospital!), and cost-effective employees (see all of the above: the hard work, persistence, ethical nature, and pride that drives us). All of that being said, a majority of autistic young adults have difficulty finding a job because we present differently to the world and employers hesitate at differences. In the United States, much of our collective concepts of adult self-worth are built around employment, as well as many social networking and friendship opportunities (Solomon, 2020). For myself, I feel a great deal of confidence and self-esteem currently because I’ve worked very hard to gain full-time employment (split between two colleges, but it still counts)! I changed careers five years ago and had difficulty finding employers to trust me with their work. I ran into supervisors who tried to have me fired through ingenuine employee evaluations. My assumption is that I made these traditional women uncomfortable by being a non-traditional woman and rather than live with this discomfort, they assumed that their discomfort at my difference was a signal they should listen to and attempt to have me removed. I fought the evaluation and won, but it’s a terrifying situation to be in to be ostracized for being different. Some maladaptive autistic behaviors are reinforced by negative experiences in school and the workforce leading to financial insecurity, which can lead to wearing clothing that is not appropriate for the workplace, unhealthy eating habits, and sleeping less due to mental health stressors. Only 58% of autistic individuals in their 20s were employed in 2015. These rates are below rates for individuals with learning and intellectual disabilities and those of ex-convicts. Employers seem to be uneducated about what autism is and how it works, and fear increased costs and declining productivity, when in many cases the opposite would be true if they hired autistic individuals. Being unemployed often results in social isolation and increased social communication deficits. For those autistic adults who are employed, it is typically for lower wages and less hours. In a 2018 CDC study they found that of autistic employees, 80% worked part-time and had a median income of $160 per week (the average American makes $961 per week). Employment challenges faced by autistic individuals affect mental and physical health of autistic people. We deserve to work and be able to support ourselves (Solomon, 2020). Traditional and alternative treatment approaches Behaviors associated with autism can be difficult to manage. When autistic individuals experience stressors, it is common for executive function to be increasingly impaired and decision making to suffer. Thus, when an autistic person is most in need of support, they are least likely to be able to secure it. There are currently no recommended pharmacological treatments for core autism features of impaired social communication and restricted or repetitive behaviors, only recommendations for how to treat symptoms such as anxiety. Even treatments for anxiety in autism are not well-researched as to how autistic brains respond differently than neurotypical brains and may need different types or levels of treatments (Aran, Harel, Cassuto, Polyansky, Schnapp, Wattad,… Castellanos, 2021). The most commonly used therapy for autism is the controversial and much maligned (in the autism community) applied behavioral analysis (ABA). There is research on both sides pointing to both the efficacy of ABA, and its abusive factors This is a topic best left for another paper, but please know that if you are interested in reading more on this topic, there is literature available. One additional support for autism that has been shown as effective in reducing emotional dysregulation and outbursts. and by extension, social communication, is exercise. Autistic individuals who exercised on a regular basis were shown to have increased emotional regulatory abilities and a reduction in internal and external behavior problems such as stereotypic behaviors, need for stimming (self-stimulating or soothing behaviors), as well as general benefits of increased strength, attention, self-esteem, and self-efficacy (Tse Andy, 2020). Modified cognitive behavioral therapy (CBT) has been used with great success for autistic individuals experiencing social anxiety. In one example of a modified CBT session, clients come for ‘café time’ and practice social skills while building group rapport among other autistic individuals. Social anxiety is a common component of decreased social ability that 50%-70% of autistic adults experience. CBT can help reduce social anxiety, which reduces other core symptoms and challenging behaviors like restricted or repetitive behaviors that are often stress-induced, while increasing social motivation. Use of modified CBT also helps improve overall mental health conditions of anxiety, depression, psychological distress, and stress. In addition to being functional, the recipients spoke favorably about their enjoyment of the CBT process, which is in stark contrast to recipients of ABA. Overall, increasing mental health and social acuity can reduce the severity of autism as a disability and allow autistic individuals to live more authentic and happy lives with reduced stress (Bemmer, Boulton, Thomas, Larke, Lah, Hickie, Guastella, 2021). One of the more controversial treatment options for challenging autistic behaviors is cannabis. Consuming cannabis can reduce hostile feelings that sometimes underlay social communication challenges and enhance interpersonal communication. Cannabidiol or CBD does not carry the psychoactive or de-motivational characteristics of THC and is being seen increasingly as a beneficial pharmaceutical option. CBD has also been shown to have antipsychotic, antiepileptic, and neuroprotective properties. There are also studies showing that individuals with autism seem to have impaired function of the endocannabinoid system of the brain and that CBD may work to restore optimal function. Research is needed comparing CBD and THC effects and find more optimal treatments for the core symptoms of autism using cannabis (Aran, Harel, Cassuto, Polyansky, Schnapp, Wattad, . . . Castellanos, 2021). Another possibility in autism therapy could be cell therapy. Many attempts at treating autism’s core symptoms have been found unsatisfactory. Researchers have found a connection between aberrant microglial activity and excessive synaptic pruning resulting in less synaptic plasticity often found in autism. Inflammation due to allergens of other chronic sources can lead to postsynaptic surplus that can also lead to autism behaviors. With aberrant microglial function in mind, it has been found that autologous cord blood cells can have a protective effect on the impairment of microglia, inflammation, and oxidative stress that researchers have associated with the development of autism traits and use of these blood cells can prompt neurological regeneration. Human CD34 positive cells release growth factors that affect brain derived neurotrophic factor production whose disruption is often associated with autism. It is possible that by using these blood cells in treatment of autism, much like they can be used in treatment of those with epilepsy, cell therapies could alter microglial function and immune system responses to assist in treatment of autism (Nabetani, Mukai, 2022). There is much yet to learn about autism in adults and research into effective treatments to improve quality of life for autistic individuals. Many of the challenges autistic people face are stressors due to the world’s reaction to our behaviors. Teaching autistic people how to better manage their mental health and behaviors and teaching the world at large more about autistic people is my goal. We can all live better lives by learning more about ourselves and each other. References Adams, R. E., Taylor, J. L., & Bishop, S. L. (2020). Brief report: ASD-related behavior problems and negative peer experiences among adolescents with ASD in general education settings. Journal of Autism and Developmental Disorders, 50(12), 4548-4552. doi:http://dx.doi.org/10.1007/s10803-020-04508-1 Aran, A., Harel, M., Cassuto, H., Polyansky, L., Schnapp, A., Wattad, N., . . . Castellanos, F. X. (2021). Cannabinoid treatment for autism: A proof-of-concept randomized trial. Molecular Autism, 12, 1-11. doi:http://dx.doi.org/10.1186/s13229-021-00420-2 Bemmer, E. R., Boulton, K. A., Thomas, E. E., Larke, B., Lah, S., Hickie, I. B., & Guastella, A. J. (2021). Modified CBT for social anxiety and social functioning in young adults with autism spectrum disorder. Molecular Autism, 12, 1-15. doi:http://dx.doi.org/10.1186/s13229-021-00418-w Cassidy, S. A., Bradley, L., Cogger-Ward, H., & Rodgers, J. (2021). Development and validation of the suicidal behaviours questionnaire - autism spectrum conditions in a community sample of autistic, possibly autistic and non-autistic adults. Molecular Autism, 12, 1-22. doi:http://dx.doi.org/10.1186/s13229-021-00449-3 CDC.gov (2020). Autism spectrum disorder (ASD) diagnostic criteria. Centers for Disease Control and Prevention. Retrieved from https://www.cdc.gov/ncbddd/autism/hcp-dsm.html on January 7th, 2021. McKenna, B. G., Huang, Y., Vervier, K., Hofammann, D., Cafferata, M., Al-Momani, S., . . . Michaelson, J. J. (2021). Genetic and morphological estimates of androgen exposure predict social deficits in multiple neurodevelopmental disorder cohorts. Molecular Autism, 12, 1-18. doi:http://dx.doi.org/10.1186/s13229-021-00450-w Nabetani, M., & Mukai, T. (2022). Future perspectives on cell therapy for autism spectrum disorder. Biocell, 46(4), 873-879. doi:http://dx.doi.org/10.32604/biocell.2022.018218 Solomon, C. (2020). Autism and employment: Implications for employers and adults with ASD. Journal of Autism and Developmental Disorders, 50(11), 4209-4217. doi:http://dx.doi.org/10.1007/s10803-020-04537-w Paul, S., Arora, A., Midha, R., Vu, D., Roy, P. K., & Belmonte, M. K. (2021). Autistic traits and individual brain differences: Functional network efficiency reflects attentional and social impairments, structural nodal efficiencies index systemising and theory-of-mind skills. Molecular Autism, 12, 1-18. doi:http://dx.doi.org/10.1186/s13229-020-00377-8 Tse Andy, C. Y. (2020). Brief report: Impact of a physical exercise intervention on emotion regulation and behavioral functioning in children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 50(11), 4191-4198. doi:http://dx.doi.org/10.1007/s10803-020-04418-2 Weir, E., Allison, C., Ong, K. K., & Baron-Cohen, S. (2021). An investigation of the diet, exercise, sleep, BMI, and health outcomes of autistic adults. Molecular Autism, 12, 1-14. doi:http://dx.doi.org/10.1186/s13229-021-00441-x  This was a research paper that I got to write for my doctorate program! Lisa R. Macafee Department of Psychology, California Southern University PSY 8700 Psychopharmacology Dr. Trachanel Cater October 18, 2021 Anxiety and Autism This paper analyses the psychological, neurological, biochemical, genetic, environmental and socio-cultural aspects of anxiety in autistic populations, with specific regard to psychopharmacological intervention. The terms autistic, autism, autism spectrum disorder (ASD), and neurodivergent are used interchangeably to refer to the autistic population. Individuals with autism often prefer identity-first language (autistic) instead of person-first language common in other disability rights movements (person with autism). I will briefly share my own experiences with anxiety and autism. I am a 39-year-old autistic female. I suffered with undiagnosed serious depression and anxiety from twelve through twenty when I finally got a diagnosis of depression and later anxiety after leaving an abusive relationship. I missed obvious signs that the relationship was troubled and exhibited magical thinking and communication deficits but am highly intelligent and have learned to mask traits that make others uncomfortable. I started studying psychology in high school and learned how to avoid scrutiny from others. No one in my circles ever thought I needed support because I was functioning in a state of constant alertness and anxiety to cover my behaviors. I assumed that I had inherited a biological predilection for anxiety because everyone in my family has struggled with it. What I now know is that we were likely generations of intelligent autistics and suffered through crippling anxiety trying to live in a world that we did not understand without getting strategies to support our needs. I learned I was autistic after my son and daughter were diagnosed autistic and started researching autism to be able to best support my children. It became obvious to me in researching that I was also autistic, and I sought a diagnosis. It has been so much easier controlling my depression and anxiety with a toolkit of responses for autism and to understand why and how I am different from neurotypical individuals. Anxiety disorders in autistic populations Autism spectrum disorder consists of significant difficulties in communication and social interactions as well as repetitive or restrictive patterns of behavior, interests of activities. Estimates vary, but the rate of autism is currently about 2% of the population and is growing. For autistic individuals who are called “high-functioning” which means the individual has higher intelligence and is verbal, being aware of their own deficits and unusual behaviors very often leads to anxiety. Intensity of anxiety in autistic individuals often seems to scale with higher intelligence as the individual tries to adapt their functioning to societal expectations. “High functioning” autistic individuals are often able to match their performance to expectations, but at a great intellectual cost of anxiety. They need to focus on and control every movement, analyze every word, and anticipate other people’s reactions. Often the autistic individuals who seem to be “high functioning” are suffering immensely from the stress of masking. As such, the term “high functioning” is reviled in the autistic communities as it is often used to deny services to individuals who are not seen as needing them as much as someone “low functioning”, an ableist and discriminatory term. Overall, autism is a very individualized disability and needs individualized and flexible care (Wiltjer, Gentry Wilkerson, Winograd, Leetch, 2021). Many factors contribute to the fact that autistic individuals often live with comorbid mental health challenges. Rates of anxiety diagnosis in autistic populations vary from 11.1% in adults to 41.9% in children, much higher than the neurotypical population (Deb, Roy, Lee, Majid, Limbu, Santambrogio, . . . Bertelli, 2021). 77.7% of autistic children also have a mental health condition and 49.1% have two or more compared to 14.1% of children without autism having a mental health disorder. Autistic individuals tend to have higher rates of mental health disorders as they get older. It is theorized that the communication challenges that are a part of autism cause increased social isolation which can contribute to depression and anxiety. To compound this, many high functioning individuals are not diagnosed with autism, but only with anxiety. If anxiety is a symptom of untreated autism, which continues to go untreated because they have a diagnosis of anxiety, treatments for anxiety alone are unlikely to be sufficient to resolve the care needs for the autistic client (Villalpando, N. 2021). Oftentimes with autism, mental health is overlooked in favor of physical care. Mental health for children and adults with autism is especially important. While health insurance often covers treatment and prescriptions, there is a demand for care that exceeds the supply and many autistic individuals are not able to navigate the health care system to get the care that they need, causing more anxiety and stress to their lives. Anxiety is more commonly diagnosed in White non-Hispanic children with autism, while children of color with autism are often diagnosed with conduct disorder or ADHD when anxiety may be a more appropriate fit. There is racial bias in those who diagnose children and White children are often treated with a more open mind to the challenges that the child experiences while children of color are given less empathy and compassion. Hispanic children are diagnosed the least with any mental health condition, pointing to structural barriers and health care systemic bias. Autistic individuals experience difficulty getting mental health care. Autistic individuals who do not receive the mental health care they need are less likely to participate in sports or work and this lack of social contact becomes a self-replicating cycle wherein they become more isolated and anxious because they do not receive the services they need to function. Anxiety is the most common diagnosis for autistic adults (Drexel university, 2021). Etiology of anxiety in autistic populations An autism diagnosis means that individuals experiences communication and social interaction difficulties and has restrictive or repetitive behaviors. While no one yet knows why autism happens, it appears to be hereditary and there are certain exposures that increase the risk of autism in utero and early childhood. These point to both genetic and epigenetic factors. There are patterns of gene expressions and genes that are more common in people with autism (Wiltjer, Gentry Wilkerson, Winograd, Leetch, 2021). Autistic individuals share significantly more genes from Neanderthals which has brought up interesting conversations of autistics possibly being the mixed-genetic descendants of Neanderthals. Some Neanderthal traits carry over and autistic individuals have physically larger brains and skulls. Commonly accepted thought is that autistic individuals have different biological necrologies than the neurotypical. Our brains are physically different and that causes different behaviors and needs (Grandin, 2014). As autistic children of higher intelligence grow older and become aware of their differences from neurotypical peers, they often experience anxiety trying to mask their autistic traits and fit in. As they get older, they often have trouble with social relationships, which causes anxiety. Living in a neurotypical world as a high functioning autistic means constantly masking, acting, suppressing self-stimulating behaviors (called stims), which all contribute to living in a state of hyper-vigilance and high levels of anxiety. For lower-functioning autistics, the behaviors they exhibit are direct responses to stresses that they cannot always articulate. Are the lights too bright? Is the desk too hard? Is the faint hum from the refrigerator that no one else notices sounding like a helicopter in its intensity and attention focus? Can the individual communicate any of this effectively to get their needs met? Autistic individuals experience the world differently from neurotypical folk and will have outbursts of behaviors when their stress levels are no longer bearable or when life demands are put on them that they cannot accommodate. If the autistic individual’s behavior causes those around them to be upset, this causes more stress and anxiety to the autistic individual who knows they are upsetting people, but often feels out of control to stop (Al-Oran, Khuan, 2021). Another contributing factor to anxiety is the fact that autistic people generally experience more lifetime social, psychological, and physical stressors than their neurotypical peers and perceive these stressors more intensely. Autistic adults are often less able to cope with stressors because they are more socially isolated, experience more loneliness, and have less social support. These heightened stressors and the body’s response to them lead to worse physical and mental health. Autistic children more frequently live in poverty and experience adverse childhood experiences. These experiences and the social reactions received because of them can bring about chronic anxiety and hypervigilance. Autistic people are more likely to have been bullied, experience social isolation, and to experience physical, sexual, and emotional abuse because of social naivete. Autistic adults are more likely to un- or underemployed, have difficulty with the justice system, and experience social stigmatization. If routines relied on to function are disrupted, this can create a spike in anxiety over what may seem inconsequential to a neurotypical individual, but for an autistic is very challenging. Add to that the communication deficits that autistic individuals experience leading to greater social challenges and less robust social support networks that increase risk of suicide, self-harm, and psychopathology. All these factors contribute to anxiety (Moseley, Turner-Cobb, Spahr, Shields, Slavich, 2021). Psychopharmacology treatment Research analysis suggests that 61.5% of autistic adults and 41.9% of autistic children use some form of psychotropic medication. Among older generation tricyclic medications, evidence of efficacy in treating anxiety of autistic populations is lacking, and side effect management for individuals with autism may be more difficult than for neurotypical populations. For these reasons, tricyclics are not recommended in treating autistics with anxiety. When looking at SSRIs for use for children with autism, there has been weak research that suggests minimal benefit and increasing evidence of harm in SSRI use. Effectiveness of use of SSRIs in autistic adults shows minimal clinical benefit, with citalopram showing the most significant benefits. Benzodiazepines could be used for short-term treatment, but not for long-term use because of their cognitive affects and addictive quality. Likewise, high doses of beta-blockers are not recommended due to side effects risks. Overall, research does not condone or refute use of medications for autistic adults. Care should be taken to weigh the possible benefits against side effects, which are often more pronounced in autistic individuals. Providers should closely monitor any medications prescribed for benefits and side effects. Individuals with autism are often overmedicated with minimal benefit and (Deb, Roy, Lee, et. all, 2021). While research in treating autistic anxiety using traditional psychopharmacological methods is lacking, some researchers are looking to non-traditional methods for atypical minds. CBD has been used increasingly among autistic populations to reduce anxiety and improve sleep, with 22% of parents and caregivers giving CBD to autistic children. CBD use in autistic populations has been shown in clinical trials to not only reduce anxiety and improve sleep for anxious autistics, but also decrease self-harm, hyperactivity, irritability, aggressiveness, depression and cognitive impairments. Given the limited legality of cannabis in much of the world, research is lacking and cannabis or CBD cannot be FDA approved because they are illegal at the federal level in the United States. There are promising signs of autistic individuals becoming more independent with the use of cannabis products. More research is needed (National organization for reform of marijuana laws, 2021). As there have been no medications proven to to improve the lives of autistic individuals, researchers are looking into more controversial and novel approaches to find solutions. Psylocibin “magic” mushrooms and ecstasy in micro-doses have been shown to have benefits for autistic individuals where traditional medications have failed. Psilocybin has shown positive results in sub-hallucinogenic doses to improve anxiety and cognition problems for autistic individuals and is likely to be FDA approved in 2022 or 2023. Similarly, ecstasy or MDMA micro-dosing has shown significant improvement when autistic individuals used to reduce social anxiety and impairments in social functioning (Ponieman, 2021). Psychotherapeutic treatment Mental health providers for people with autism often function as a life coach. Therapists often help an autistic person sift through the daily pressures and stresses that life brings and strategize ways to move forward that are overwhelming to an anxious autistic person. Many autistic individuals face additional barriers in accessing mental health services due to the nature of their disability. To reduce these barriers, it is suggested that clinicians try to reduce crowded environments, loud noise, bright lights, and long wait times or offer remote appointment services, which are often preferred for comfort and feelings of safety. Education on autism and encouragement to respond with flexibility instead of rigid responses can reduce fear of stigma and increase participation from autistic individuals with anxiety. Clinicians working with autistic populations need to be trauma-informed and respond with knowledge of how adverse childhood experiences common in autistic children can affect individuals with care not to re-traumatize them in treatment. Many mental health therapies that work well in traditional populations such as cognitive behavioral therapy will often need to be adapted for use in autistic population to be functional and prevent increased anxiety to the client. Clinicians should be aware of autism diagnostic criteria when treating seemingly non-autistic individuals with anxiety, especially women, who are underdiagnosed autistic, as anxiety is often a symptom of untreated autism. There are autistic-specific accommodations that can be provided and strategies for self-help when the individual knows they are autistic that dramatically reduce anxiety. Delays in identification of autism often lead to increased anxiety that is more difficult to treat (Roy, 2021). This paper would not be complete without discussing the debate about ABA, or applied behavioral therapy. ABA is controversial and is generally reviled among autistic advocacy groups which describe it as dehumanizing and abusive. I believe that elements of ABA can be utilized without maintaining the discrete trial and compliance components of the original ABA. ABA can be used to help autistic individuals break up anxiety-producing tasks into smaller step-by-step routines and teach replacement behaviors for undesirable ones. For ABA to be ethical, the autistic individual needs to be involved in goal creation and listened to if they experience distress in treatment. Speech and occupational therapies are often used with autistic populations and can help reduce anxiety (Wiltjer, Gentry Wilkerson, Winograd, Leetch, 2021). Treating anxiety in autism required multi-modal care. For example, while increased social media use among neurotypical teens has shown greater associations with depression and anxiety, when autistic teens engage in social media, if functions to reduce their overall anxiety. Autistic teens with anxiety appear to use social networking sites to build community, connect with friends in authentic ways, and have fun. This suggests autistic neurology is different in many ways from their neurotypical peers. (Lunn, Cogdon, 2021). Social-communication challenges are one of the contributing factors in anxiety among autistic individuals and treatment should focus not only on therapeutic interventions but also on helping the autistic individual find ways to involve themselves in a sense of community. Participating in employment or even in support groups has been shown to help autistic individuals increase their social skills and decrease their anxiety. Assisting individuals with interpersonal challenges and teaching social skills as they navigate the work and social realms will be important for their adaptation to being more involved in the community. Being involved in the community contributes to higher emotional intelligence, and both community involvement and emotional intelligence lead to reduced anxiety and higher quality of life. Particular care should be made to assist autistic individuals in periods of transition, which is often one of the most stressful times of life for autistics. Both support groups and social skills groups have been found to help autistic adults with anxiety by establishing a sense of belonging, a place where they can be understood, and see reflections similar to themselves in others to reduce alienation (Flores, Delariarte, 2021). Autistic brain differences are not well understood. Traditional therapeutic methods for anxiety should be considered, but one treatment that has shown effectiveness in autistic populations is exercise. Exercise often provides autistic individuals opportunities for community engagement, to be part of a group class, competitive sport, or hobby, and gives many structured time outside in the sun. All of these factors are especially beneficial for autistic individuals. In many exercise environments social interactions are either minimal, structured, or conversation topics can surround the exercise instead of personal topics. This removes much of the stress of social interactions for autistic individuals. Some have found that exercise reduces cognitive difficulties, which makes it easier to converse with others, which reduces anxiety. We all know that exercise is beneficial, but for autistic folks, it can be important than for others! (Conboy, 2021). One of the more important treatment needs for autistics with anxiety is crisis response care. Individuals need quality of care options in crisis beyond calling 911 or going to an emergency room where staff have little to no training in how to work with autistic adults. There need to be resources that autistic adults with anxiety can utilize to deal with mental health issues where they will get appropriate care. This is especially needed for autistic individuals of color, who are often misunderstood and experience racial bias in health care from a majority White health care team. Cultural competence and autism education are needed in our healthcare systems for effective care. (Drexel university, 2021). Research gaps Much research is needed as to effective treatments of anxiety for individuals with autism, adults with autism, and women with autism (Wiltjer, Gentry Wilkerson, Winograd, Leetch, 2021). While many autistic individuals are using psychotropic medications, little research has been conducted specifically on the use of prescriptions in autistic neurology and how they may deviate in effect from neurotypical populations. It is likely that autistic individuals are overmedicated without gaining significant benefits. While many SSRIs are used to treat anxiety in autistic populations, there is minimal and inconclusive research as to their efficacy. More research is needed not only to find more effective prescription drugs to treat autistic anxiety, but also to determine why traditional medications have limited efficacy. At this point we are left to conjecture about differing neurology requiring substantially different medical approaches, but there is not research explaining how or why (Deb, Roy, Lee, et. all, 2021). More research is needed in treating autistic anxiety with cannabis, CBD, psylocibin, and MDMA. Initial studies have found better responses from autistic individuals using micro-doses of these substances that have been shown from SSRIs and other FDA approved prescriptions that work well for neurotypical populations but appear to have less efficacy for autistic populations (National organization for reform of marijuana laws, 2021). References: Al-Oran, H., & Khuan, L. (2021). Predictors of parenting stress in parents of children diagnosed with autism spectrum disorder: A scoping review. The Egyptian Journal of Neurology, Psychiatry, and Neurosurgery, 57(1) doi:http://dx.doi.org/10.1186/s41983-021-00345-w Conboy, M. (2021). How trail running helped ease anxiety from autism. Bow Valley Crag & Canyon Retrieved from http://proxy1.calsouthern.edu/login?url=https://www.proquest.com/newspapers/how-trail-running-helped-ease-anxiety-autism/docview/2592770238/se-2?accountid=35183 Deb, S., Roy, M., Lee, R., Majid, M., Limbu, B., Santambrogio, J., . . . Bertelli, M. O. (2021). Randomized controlled trials of antidepressant and anti-anxiety medications for people with autism spectrum disorder: Systematic review and meta-analysis. BJPsych Open, 7(6) doi:http://dx.doi.org/10.1192/bjo.2021.1003 Drexel university (2021). National autism indicators report - high rates of mental health conditions and persistent disparities in care. 2021, Sep 01. Targeted News Service Retrieved from http://proxy1.calsouthern.edu/login?url=https://www.proquest.com/wire-feeds/drexel-university-national-autism-indicators/docview/2567973257/se-2?accountid=35183 Flores, D. G., & Delariarte, C. F. (2021). Community participation as mediator of trait emotional intelligence and health-related quality of life of adults with high-functioning autism. North American Journal of Psychology, 23(3), 491-507. Retrieved from http://proxy1.calsouthern.edu/login?url=https://www.proquest.com/scholarly-journals/community-participation-as-mediator-trait/docview/2577808179/se-2?accountid=35183 Grandin, T. (2014). The autistic brain: helping different kinds of minds succeed. Boston, New York: Mariner Books, Houghton Mifflin Harcourt Lunn, S., & Cogdon, K. (2021). Autistic teens ‘at ease’ on internet. The Australian (Online) Retrieved from http://proxy1.calsouthern.edu/login?url=https://www.proquest.com/newspapers/autistic-teens-at-ease-on-internet/docview/2595963608/se-2?accountid=35183 Moseley, R. L., Turner-Cobb, J. M., Spahr, C. M., Shields, G. S., & Slavich, G. M. (2021). Lifetime and perceived stress, social support, loneliness, and health in autistic adults. Health Psychology, 40(8), 556–568. https://doi-org.csu.idm.oclc.org/10.1037/hea0001108.supp (Supplemental) National organization for reform of marijuana laws (2021). Survey - more than one in five U.S. caregivers report providing CBD to treat autistic symptoms. 2021, Oct 15. Targeted News Service Retrieved from http://proxy1.calsouthern.edu/login?url=https://www.proquest.com/wire-feeds/national-organization-reform-marijuana-laws/docview/2582100040/se-2?accountid=35183 Ponieman, N. (2021). Magic mushrooms and ecstasy: New treatment for autism spectrum disorders? Benzinga Newswires Retrieved from http://proxy1.calsouthern.edu/login?url=https://www.proquest.com/wire-feeds/magic-mushrooms-ecstasy-new-treatment-autism/docview/2590349567/se-2?accountid=35183 Roy, A. (2021). How can psychiatrists make mental health services more accessible for people with autism? BJPsych Open, 7(6) doi:http://dx.doi.org/10.1192/bjo.2021.1036 Villalpando, N. (2021). Is it autism? mental illness? both? how to navigate double diagnosis. Austin American Statesman Retrieved from http://proxy1.calsouthern.edu/login?url=https://www.proquest.com/newspapers/is-autism-mental-illness-both-how-navigate-double/docview/2581626315/se-2?accountid=35183 Wiltjer, R., Gentry Wilkerson, R., Winograd, S. M., & Leetch, A. N. (2021). Autism spectrum disorder in the emergency department. Emergency Medicine Reports, 42(15) Retrieved from http://proxy1.calsouthern.edu/login?url=https://www.proquest.com/scholarly-journals/autism-spectrum-disorder-emergency-department/docview/2554269069/se-2?accountid=35183  This was a research paper that I got to write for my doctorate program!
Cognition, emotion, and motivation in gender diversity Lisa R. Macafee California Southern University PSY 8724 Cognition, Emotion and Motivation Dr. Debra Pearce August 15, 2021 Cognition, emotion, and motivation in gender diversity This paper discusses how cognition, emotion, and motivation affect the construction of gender. This paper will discuss the personal, environmental, and sociocultural components involved with gender diversity. Gender diversity includes any gender identity outside of cisgender (identifying as the gender assigned at birth). Transgender identities, often called “trans” for short, include anyone who does not identify 100% with the gender assigned at birth and can include trans men, trans women, non-binary, gender fluid, 3rd gender, agender, gender non-conforming, and pangender identities. Approximately 0.6% of adults and 2.7% of adolescents in the United States identify under the transgender umbrella, with younger individuals coming forward and an increasing number of non-binary individuals (Bowman, Casey, McAloon, Wootton, 2021). Trans and gender diverse are used interchangeably in this paper. I am writing about gender diversity because I identify as non-binary and work with the LGBTQIA+ population to provide supports for the community. Cognition around gender Thankfully, people are broadening their understandings of gender and are beginning to see sex and gender more broadly and less on the binary. Cisgender heterosexual individuals have the least cognitive understanding of gender and sex as fluid or complex and tend to define more based on biological terms, while transgender and gender diverse individuals understand gender in more complex terms in sociocultural context. Younger individuals perceive gender more as a spectrum when compared to older individuals who think more in binary terms that are explicitly tied to the sexual parts an individual possesses. The more power and privilege a group has, the more likely they are to hold in place discriminatory systems that benefit them. For example, White people and men are both more likely to hold essentialist beliefs about sex and gender and are more likely to attribute gendered traits to genetics. Groups who have been disenfranchised are more likely to question the same hierarchies and critically engage with them, leading to a more nuanced understanding of the hierarchies of gender and sex. Minoritized people are more likely to think about sex and gender in inclusive terms, such as: sex and gender may not match, gender assigned at birth may be different from gender identity, individuals may move between genders, be somewhere in between, or be no gender. Thinking more inclusively better ensures that others are not harmed by the individual’s definitions and excluded from their conceptions and resists biological essentialism (Schudson, Beischel, van Anders, 2019). There are many gendered expectations for those who are gender diverse that can be confusing at times. For myself, I remember clearly being told in high school that I was a “dude with ovaries” and that I should just admit that I was a lesbian, because clearly a person assigned female at birth (AFAB) who was gender non-conforming must be gay. The conflation of gender and sexuality is rampant both within queer communities and cisgender-straight communities. People often see atypical gender presentations such as a feminine man or masculine woman and assume they are gay. This assumption is sometimes accurate, but often it is not. Gender and sexuality are not tied together, but our socialization tells us it is. Trans individuals are expected to be straight and hyper-gendered. Being trans and gay confuses people who do not experience the gender dysphoria present in many trans individuals pre-transition. Many trans individuals continue to experience gender dysphoria during and after transition. These individuals may have adopted the idea that they need to transition all the way to the opposite binary gender assigned at birth and that an in-between gender identity is somehow unintelligible. There is pressure that to be truly trans, one must conform to society’s expectations of “male” and “female”. To avoid criticism, individuals must adopt a cisgender mask to be palatable and not confuse others. For trans folk, “passing” is a privilege and difficulty. Dealing with microaggressions and aggression causes gender diverse folk to constantly question themselves; ‘Should I try to pass more to avoid harassment?’; ‘Should I live “out” more to advocate for trans rights?’; ‘Is it my responsibility to educate every person who misgenders me or tries to convince me I’d be happier as a cisgender person?’ Existence is an act of rebellion for many of us gender benders, and it is exhausting. (Jones, 2021). Many trans and non-binary individuals experience some degree of gender dysphoria. Gender dysphoria is experienced when there is an incongruence between the gender assigned at birth and the gender identity an individual holds that causes them distress. Individuals experiencing gender dysphoria may feel uncertainty, stigma, guilt, and body dissatisfaction on their journey to living more authentically as their authentic gender instead of performing as the gender they were raised to be. The feeling that the experience of gender a person has is wrong is often accompanied by increased levels of anxiety, depression, self-harm, and suicidality. Many individuals are able to resolve the gender incongruence that causes distress by gender-affirming practices such as social transition, hormone blockers for adolescents, hormone therapy, and surgery. Others may also need therapy to resolve the internalized gender issues. When a person has been raised from infancy to be a certain gender with certain gendered personality traits and they do not feel that is an authentic way of being for them, it is often not simply a light switch to be turned on and off from one gender presentation to the other, it requires a great deal of processing to be able to exist in a new presentation to the world from the previous indoctrinated presentation. I have been in my gender journey for only a few years as before that I simply attempted to be what I was told I should be. I have always known I was different from others, and a “tomboy”, but didn’t have the vocabulary to process what that might mean for me until recently (Bowman, Casey, McAloon, Wootton, 2021). Emotion and gender One of the emotional factors that most people who are not gender diverse don’t understand is the constant presence of fear. Fear of being discovered, fear of sharing one’s identity with someone and being rejected for it, fear of persecution, fear of the unknown fear of oneself. One of the most harmful fears is the fear of getting effective and appropriate medical and psychological care. Many trans individuals navigate shame and social rejection just for living as who they are. Seeking out mental health support often results in a gender dysphoria diagnosis and pathologisation leading to pressure to live as the gender assigned at birth or 100% the opposite gender assigned at birth instead of mental health support for the depression and anxiety that is often the result of being different. Not enough therapists are adequately trained to work with gender diverse clients (Jones, 2021). Many people, both gender diverse and cisgender, have a great deal of internalized cis-sexism; the unconscious belief that being cisgender is superior to being transgender. Leading to this outcome are the heightened levels of physical, verbal, and sexual assault that transgender and gender non-conforming (TGNC) individuals experience compared to their cisgender peers. TGNC folks also experience higher levels of mental and physical health problems and higher levels of substance abuse as a coping methos compared to their cisgender peers. This is understandable considering the amount of minority stress and cis-normative frameworks that TGNC people experience. When TGNC people attempt to educate those around them who microaggress against them by imposing cis-normative expectations, this often leaves the TGNC individual exhausted and anxious after being vulnerable with people who often have hostile and negative responses. I have experienced this so many times now that instead of calling someone out in the moment, I have begun offering LGBTQIA+ Foundations trainings to faculty, staff, and students at my campuses so those who do want to be better can. It is my intention by speaking up loudly and clearly and getting administrative and mainstream support across campus that the culture of the institutions that I work in will change enough to better support TGNC students and staff and suppress anti-trans hostility (Ehlinger, Folger, Cronce, 2021). Non-binary individuals often feel pressure from the LGBTQIA+ and straight communities to try to “pass” as male or female, being neither often makes people uncomfortable. I identify as non-binary and the experience of having my very existence making people uncomfortable makes me feel anxious and pressure to conform, it is difficult not to internalize that making people uncomfortable is problematic on my part, and not their responsibility to accept more diverse people. I am left with a sense of “otherness” that I am unable to shake, a feeling that I will never be part of any group, because I do not fit into their molds. I realize that as a White person, I experience a greater privilege than TGNC people of color. It becomes clear that TGNC people of color are some of the most disproportionately impacted people in the Unites States because they face cis-sexism in their cultural communities and racism in the queer communities. The feelings of alienation and otherness from most communities leaves TGNC individuals at high risk for substance abuse and self-harm, increasingly so with added marginalized statuses such as race, ethnicity, immigration status, socio-economic status, (dis)ability, and sexual minority status (Ehlinger, Folger, Cronce, 2021). Motivation and gender diversity For some to get gender treatment, they must conform to binary gender stereotypes and be transgender to qualify for physical and mental health services. This pressure to fit into a false binary existence to get care causes motivation to be hyper-masculine or hyper-feminine, which can cause its own gender dysphoria (Jones, 2021). For individuals who are delayed in their gender and sexuality exploration and identity formation, they often experience negative mental health impacts (Hawke, Hayes, Darnay, Henderson, 2021). I am 39 years old and only started to think about my own gender four years ago when I attended a presentation that discussed a term I had not heard before, transgender and gender non-conforming (TGNC). This identity label changed my life. I had lived with a baseline level of anxiety and depression and lack of belonging my entire life, and this term just explained why. While I do not identify as a female, as I was assigned at birth, neither do I identify as male. I identify as outside of those repressive roles and cannot fathom how others truly feel safe in those identity boxes. The moment I decided it was okay to be atypical in my gender presentation approximately two years ago was when my confidence started to scale upwards, and my motivation increased. I collected others involved in gender justice, organized groups, gave trainings, and started multiple services at the colleges I work at for students like me (and those not like me, but struggling with similar fears and anxieties). I recognize the suffering in others and am more able to take action to lessen such suffering now that I have accepted myself. It’s only been four years since I started to think about how the gender role expectations that I had tried to live inside of for my adult life were stifling and depressing. In those four years my career has blossomed as others see drive and confidence instead of fear and nervousness. Personal Factors Many gender diverse individuals end up losing their positionality in their family of origin as certain members are too rigid in their beliefs or strict in whom they accept to allow a non-binary family member a proverbial seat at the table. Gender diverse individuals often lose financial supports, familial supports, and socio-emotional supports if they dare to express themselves as who they are. The real or perceived fear of losing these supports may cause gender diverse individuals to attempt to conform to cisgender expectations to avoid losing social and financial assets (Jones, 2021). There has been talk in conservative media outlets claiming that 80% of gender expansive children will grow up to be cisgender in adulthood. The flawed research studies that promote this idea warn parents of trans children not to provide life-saving gender-affirming treatments to youth because their experience of being transgender is a phase. There are many personal factors that account for individuals who did receive gender-affirming treatments and regret it such as a realization that they are non-binary instead of trans-binary, the cost of living out and trans was too much for the individual to bear, and discrimination, among only a few of the reasons people de-transition that are not “a phase”. However, more recent research suggests that 96% of all trans youth continue to identify as gender diverse into adulthood. Gender-affirming social transition such as name and pronoun change, clothing, hair, and demeanor, have shown to save lives and increase general well-being for gender diverse individuals. Those who socially or medically transition are more likely to have personal factors of family and peer support, be White, and have a high socio-economic status (Ashley, 2021). An additional personal factor that influences an individual’s desire to present as gender non-conforming for those assigned female at birth (AFAB) is internalized sexism. Many AFAB individuals have internalized so much negativity and associations of weakness about femininity that they cannot stand to associate with it. For some, to be female is to be vulnerable, more emotional, less successful, more domestic, and associated with being a caring nurturer instead of an independent provider. These individuals may present as “butch” lesbians, trans men, or other identities. They can bring a high degree of sexism to the queer community and discriminate against feminine lesbians, trans women, feminine gay men, and others, often their own partners (Ivey, 2017). Environmental Influences Environmentally speaking, there is a serious safety concern when out in society as a gender diverse person. When someone doesn’t fit into the expected binary categories, people who are uncomfortable with non-binary genders often react with hostility. This can range from micro-aggressions to physical assault. I was harassed and called names daily because I did not conform to gender expectations and took to carrying a knife with me to school because I did not feel safe. Some trans folk are told they make others uncomfortable and are barred from working with vulnerable populations such as foster youth and domestic violence survivors. This is especially unfortunate because a high percentage of foster youth are gender non-conforming, which is often why they are in foster care in the first place (Jones, 2021). There is an upsetting amount of cissexism and racism in queer and trans places that further marginalizes gender diverse people of color. Queer communities were mostly built around the work of White gay men, and many queer spaces are not as welcoming to gender minorities as they are to sexual minorities. The racialization of trans individuals of color impacts their experiences and differentiates them from their White trans peers, often making it difficult to find communities where they feel they belong. Being a trans individual is marginalizing and being a trans individual of color is exponentially marginalizing due to the increase in factors that may bring discrimination from different groups. Trans people of color are some of the most marginalized people in the United States and benefit from being in environments that are actively anti-racist along with anti-cissexism and White allies that do their homework to learn about the disproportionate impacts on queer people of color (Simms, Nicolazzo, Jones, 2021). For individuals whose gender does not conform to what they were assigned at birth, typically referred to under the transgender umbrella, the rates of PTSD are significantly higher than the general population with trans rates of PTSD between 17.5%- 45% compared to 5%-10% for the general population. This heightened rate of PTSD is likely due to the increased risk of victimization and trauma that trans people experience living in a hostile social environment of discrimination, rejection, harassment, non-affirmation, internalized transphobia, expected rejection, and concealment. When someone lives outside their gender expectations and they experience anti-transgender bias and non-affirmation, this is traumatizing to the individual who is not only feeling rejected and as though they don’t have a right to exist, but also because the more negativity around their gender they experience, the more they are likely to internalize transphobia and negative feelings around their gender themselves. The more the individual has internalized transphobia, the less regulatory functions their brain is able to use to protect their self from the effects of trauma and the more severe their PTSD symptoms tend to be. It is crucially important that trans individuals find environments that validate and celebrate their gender identity for them to reduce their internalized transphobia (Barr, Snyder, Adelson, Budge, 2021). Sociocultural Components Being gender diverse in a culture that only approves of the cisgender narrative creates mental stress. The two typically accepted cultural spaces for gender diverse individuals are to put on a cisgender mask and bury their authentic gender diverse self or transition to the opposite binary gender and be accepted in some queer communities but live in a marginalized and dangerous space. For people choosing a binary trans experience, they are often exposed to the word by their physical characteristics as transgender. For those trans folks who are “passing” (viewed as cisgender the gender they present as), when people learn of their transgender identities, some individuals may feel as though they have been lied to, which produces agitation and resentment. Few spaces allow for identities in between the binary gender expectations (Jones, 2021). Many queer activists believe that trans folk should be “out” to the world as trans to propel the cultural acceptance of trans identities, but living publicly as a gender diverse individual brings safety risks and discrimination, exponentially so if the trans individual lives in intersecting identities of racial, socioeconomic, or (dis)ability status. Many gender diverse individuals feel pressure to represent transgender identities in the world while at the same time negotiating their physical safety (Jones, 2021). Conclusion I am completing my PsyD to provide gender-affirming therapy services to trans and gender diverse individuals. I know from experience how frustrating it was when I asked my therapist about non-binary and she blew me off. I know how discouraging it was when I asked my health care provider about being intersex and having her tell me that “if you were a hermaphrodite, you’d have a penis”. Please note the two very different words used of “intersex” and “hermaphrodite” (an offensive and dated term). The mental and physical health communities are grossly undereducated about queer issues and uncomfortable providers often come off hostile to individuals who are just trying to survive. I know that when people feel supported and validated in their intersecting identities, they have higher senses of well-being, are more successful, and exhibit less mental health struggles. I want to be part of the solution. References: Ashley, F. (2021). The clinical irrelevance of “desistance” research for transgender and gender creative youth. Psychology of Sexual Orientation and Gender Diversity. https://doi-org.csu.idm.oclc.org/10.1037/sgd0000504 Barr, S. M., Snyder, K. E., Adelson, J. L., & Budge, S. L. (2021). Posttraumatic stress in the trans community: The roles of anti-transgender bias, non-affirmation, and internalized transphobia. Psychology of Sexual Orientation and Gender Diversity. https://doi-org.csu.idm.oclc.org/10.1037/sgd0000500.supp (Supplemental) Bowman, S. J., Casey, L. J., McAloon, J., & Wootton, B. M. (2021). Assessing gender dysphoria: A systematic review of patient-reported outcome measures. Psychology of Sexual Orientation and Gender Diversity. https://doi-org.csu.idm.oclc.org/10.1037/sgd0000486 Ehlinger, P. P., Folger, A., & Cronce, J. M. (2021). A qualitative analysis of transgender and gender nonconforming college students’ experiences of gender-based discrimination and intersections with alcohol use. Psychology of Addictive Behaviors. https://doi-org.csu.idm.oclc.org/10.1037/adb0000752 Hawke, L. D., Hayes, E., Darnay, K., & Henderson, J. (2021). Mental health among transgender and gender diverse youth: An exploration of effects during the COVID-19 pandemic. Psychology of Sexual Orientation and Gender Diversity, 8(2), 180–187. https://doi-org.csu.idm.oclc.org/10.1037/sgd0000467 Ivey, G. (2017). Gender mobility in the countertransference: An autoethnographic investigation. Counselling & Psychotherapy Research, 17(1), 42–52. https://doi-org.csu.idm.oclc.org/10.1002/capr.12101 Jones, D. B. (2021). De-colonising My Trans Body: Fanon and the masks I have worn. Existential Analysis: Journal of the Society for Existential Analysis, 32(2), 322–332. Schudson, Z. C., Beischel, W. J., & van Anders, S. M. (2019). Individual variation in gender/sex category definitions. Psychology of Sexual Orientation and Gender Diversity, 6(4), 448–460. https://doi-org.csu.idm.oclc.org/10.1037/sgd0000346 Simms, S., Nicolazzo, Z., & Jones, A. (2021). Don’t say sorry, do better: Trans students of color, disidentification, and internet futures. Journal of Diversity in Higher Education. https://doi-org.csu.idm.oclc.org/10.1037/dhe0000337 Autistic burnout By Lisa Macafee What does autistic burnout feel like for me? It’s different for every autistic person, so I won’t pretend mine is typical. Today is Wednesday. I started a new job last week and now work two part-time jobs for a total of 40 hours split between them. I have been navigating new procedure (in person!), new people, have been trying to be approachable and bond with new co-workers, and perform my other job responsibilities well, be a good mom, a loving wife, a competent student, and keep the house in order. This Monday, I had Locke in the car ready to take him to daycare as Ryan left with Rowan… and my car wouldn’t start. The panic rose in my chest as I did everything I could to start the car. Eventually, I was able to get it going, but it kept having the issue, so I called on my way to work on Tuesday to arrange to drop if off after work. I dropped off the car after work Tuesday, pulled a car seat out and hauled it over to the rental agency, rented a car, put the car seat in, picked up Locke, and got home around 5pm. Today, I took Locke to daycare, drove to work, worked (and had some delightful but intense conversations with co-workers), went home to pick up the recalled charger, took the car seat out, took the rental back, picked up my car after being fixed, but was told they forgot to order the replacement part for the recalled charger and could I stop by tomorrow to get it. This was the third time I brought my car in for the same recall, and they are telling me to come back again. This is the moment. Too many new things. Too much management of feelings. Too many physical tasks. I immediately wanted to cry, which I felt the need to furiously repress, because I have internalized that I can’t show weakness. Without an ability to vent the frustration, I get hot with anger, which I also repress, because I’ve internalized that angry women are hysterical and not to be taken seriously. My brain just skids out like the tires losing traction on the road. My speech drops to monosyllabic responses, my affect goes flat, and my body gets shaky and uncoordinated. It feels like there are a swarm of bees in my head that I can’t hear through or think around. I often feel unsafe to drive in these situations. I get a plummeting sadness. Then I go pick up Rowan and put on my “mom” face. Put the car seat back in. Be happy, kind, loving. Then Locke is having his own autistic burnout because he has been in daycare longer than normal and his routines are out of whack and he is screaming, kicking, and crying at us. I get it, kid, I get it. It takes everything I have to be calm. To not react with anger. To hold him in his anger and let him express it so he can feel better. Put the kids to bed. Be so mentally and physically exhausted that all I can do is this and then sleep. When I get to this place, I do not feel able to speak about anything, but I feel a compelling need to write it out. So here we are. As Nicholas Cage said, “OH, NO, NOT THE BEES! NOT THE BEES! AAAAAHHHHH!”  Coping with Disability |
Hello friends! I would like to publish writings from myself and other people with autism as snapshots of how autism has affected them, since there are so many misconceptions and confusions about adults with autism.
Some background: I completed a 12 unit certificate program to be able to serve autistic students and am angry at how the program focused only on little boys as autistic and completely left out adults, the trans autistic population, and girls/ femmes/ women autistics. I am currently pursuing a PsyD to do more research on autism and gender. Please contact me if you would like to add a story! If so, please send me your piece, publish name, title, and an image (can be a picture related to your content, your picture, an autism meme, etc). I am interested in publishing this collection, because people don't know enough about us (but sure do assume a lot). Also on Facebook! AuthorLisa Macafee, autistic counselor with a hankering for social justice. Archives
March 2024
Categories |




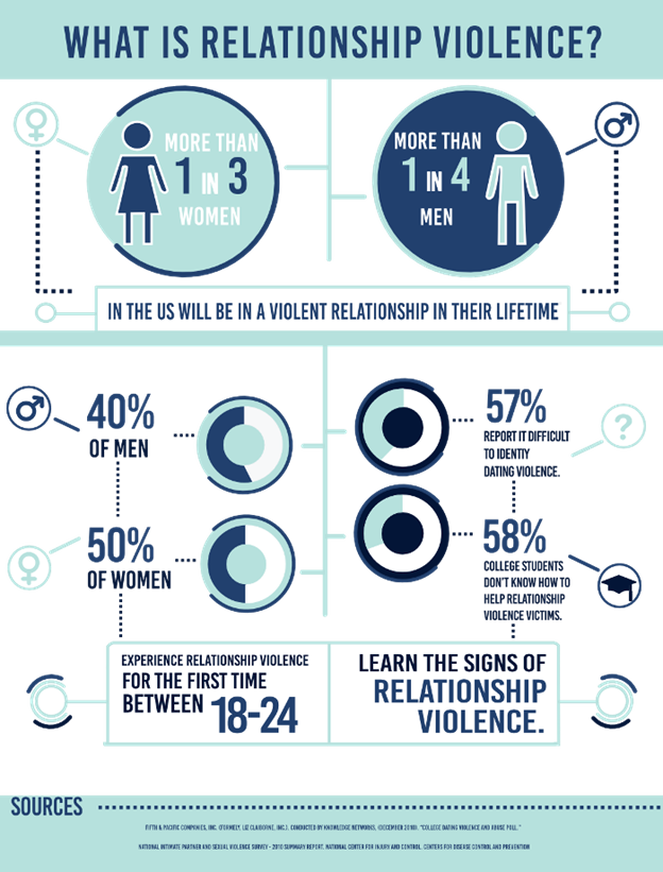

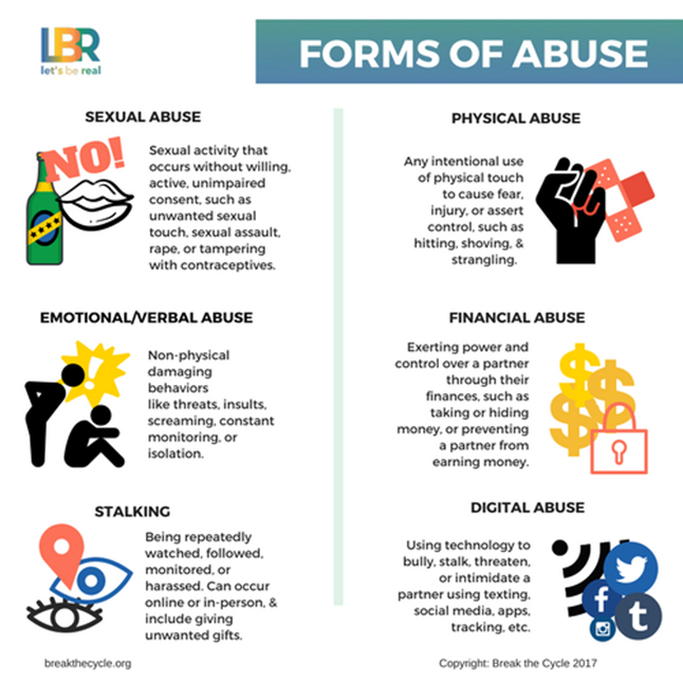
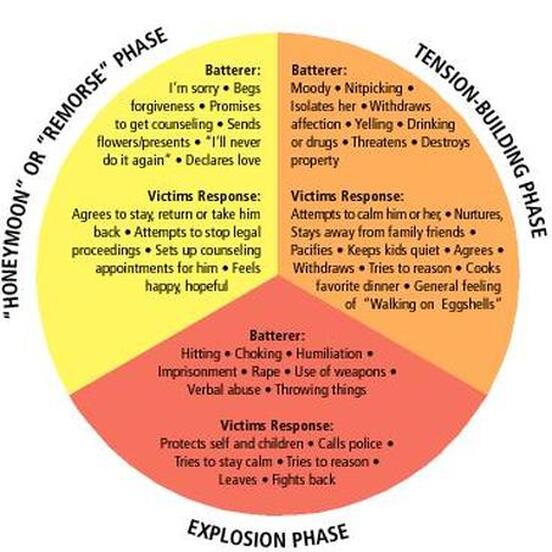
 RSS Feed
RSS Feed