 AUTISM AND TRANSGENDER IDENTITIESby Lisa Macafee Multiple studies point out an overrepresentation of autism among people seeking gender affirming care (Heylens et al., 2018; Jones et al., 2011; Nobili et al., 2018) and non-binary and transgender identities among autistic people (George & Stokes, 2018; Kirkovski et al., 2013; Strang et al, 2014). Gender-affirming care seekers are have been found to be autistic at eight to eleven times the rate of the cisgender population. Depending on the measurement tools used (Ehrensaft, 2018; Kallitsounaki & Williams, 2022) and some autistic AFAB people express concern that their autism conflicts with a traditional female gender identity (Allely, 2018). While only 0.6% of United States adults identify as transgender (Bowman et al., 2022), studies reporting rates of gender non-conformity or gender diversity among autistic people are reported near 15% (Kallitsounaki & Williams, 2022), yet there has been little summarization of data from different research projects linking them together, which is the intent of this literature review. The first question synthesized the research on autism and gender diversity. Theme One: Rates of Gender Diverse People with Autistic Traits Gender diverse people, which includes transgender, non-binary, and gender non-conforming people, have autistic traits disproportionately from the general population (Heylens et al., 2018; Maroney & Horne, 2022; Strang et al., 2021). In fact, between 23% (Strang et al., 2021) to 36% (Nobili et al., 2018) to 68% (Thrower et al., 2019), to 75% of gender-affirming seeking care patients show autistic traits (Ehrensaft, 2018). Studies vary on frequency, but people with gender identity disorder or gender dysphoria are autistic between six (Heylens et al., 2018; Pinna et al., 2022; Strang et al., 2023), seven (Strang et al, 2014), eight (Ehrensaft, 2018), or eleven times (Kallitsounaki & Williams, 2022) more frequently than the general population. Overall, 31.25% of gender-affirming care seeking AMAB and 22.22% of AFAB people were found to have elevated autistic traits (Heylens et al., 2018). While only 11% (Kallitsounaki & Williams, 2022) to 23% (Thrower et al., 2019) have an autism diagnosis, transgender people exhibit high levels of anxiety, depression, and substance use common among undiagnosed autistic adults (Mezzalira, 2022; Pinna et al., 2022). Theme Two: Number of Autistics with Gender Diversity Many studies demonstrate the relationship between gender diversity and autism (Attanasio et al., 2021; Cooper et al., 2022; Davies, 2023; Ehrensaft, 2018; Kallitsounaki & Williams, 2022; Kirkovski et al., 2013). Autistic people have higher rates of gender dysphoria (Lim et al., 2022; Thrower et al., 2019), gender non-conformity (Strang et al, 2014), and non-heterosexual orientations (Attanasio et al., 2021), possibly due to their distance from traditional gender identity (George & Stokes, 2018). Between 4.5% (Libsack, 2021) to 13% (Strang et al., 2023), to 15.4% (Kallitsounaki & Williams, 2022; Maroney & Horne, 2022; Strang et al., 2021) report transgender or non-binary identities, which is more than seven times as the neurotypical population (Tankersley, 2021; Thrower et al., 2019). Autistic people often understand gender outside of typical binary norms or male or female and often express more diverse genders such as non-binary or gender fluid identities (Kallitsounaki & Williams, 2022), and disproportionately experience gender stress or gender dysphoria (Ehrensaft, 2018). Autistic people have expressed a need to more broadly understand their interrelated gender and autistic identities and have expressed acute distress when their bodies do not match their gender identity (Cooper et al., 2022). That being said, there is also a growing push to embrace a need to experience gender euphoria, to help transgender and non-binary autistic people feel authentic joy in their bodies and identities when gender identity is embraced (Strang et al., 2023). Theme Three: AFAB Autistic Transgender Rates While both AMAB and AFAB autistics are more likely than cisgender peers to endorse feelings of gender non-conformity, AFAB autistics do so at higher rates than their autistic male peers (Davies, 2023; Jones et al., 2011) or neurotypical female peers (Kallitsounaki & Williams, 2022). Autistic AFAB people exhibit greater typical male patterns of cognition and behavior than non-autistic AMAB people (Jones et al., 2011) and experience inconsistency between their gender and physical bodies, as they report higher levels of male-typical hormone conditions (Kirkovski et al., 2013). The extreme male brain theory suggests this is due to androgen exposure in the womb that both increases masculine hormones and autism rates (McKenna et al., 2021; Nobili et al., 2018) and contributes to feelings of gender incongruence for AFAB autistics (Saffie & Bauerle, 2023). Roughly 30% of transmen (people AFAB who identify with the male binary gender identity) exhibit an autistic profile, which is eleven times as many autistic traits as compared to averages of cisgender men (Jones et al., 2011), and 45% (Nobili et al., 2018) to 68% of transmen show signs of autism (Kallitsounaki & Williams, 2022). AFAB autistics have increased risk of suicidal behaviors, psychiatric conditions, central sensitivity syndromes, and quality of life (Davies, 2023), which may be related to increased gender non-conformity (Allely, 2018). Discussion There does seem to be a consensus that autism and transgender identities are often related and occurring simultaneously at disproportionate rates (Strang et al., 2023; Thrower et al., 2019), but estimates vary between three to eleven times the rate of autism in transgender populations (Heylens et al., 2018; Kallitsounaki & Williams, 2022; Pinna et al., 2022) and up to 15% of the autistic population identifying as transgender (Maroney & Horne, 2022; Thrower et al., 2019). Given that transgender autistic people have lower quality of life than neurotypical transgender people (Mezzalira, 2022; Tankersley, 2021) and gender identity is a core part of self-understanding and shapes a person’s interactions with the world (Walker, 2021), this is an important issue to address. In addition to autism being overrepresented in transgender populations, transgender men and non-binary AFAB people have the most autistic traits from any other group (Pinna et al., 2022).  ReferencesAllely, C.S. (2019), Understanding and recognising the female phenotype of autism spectrum disorder and the “camouflage” hypothesis: a systematic PRISMA review, Advances in Autism, 5(1), 14-37. https://doi.org/10.1108/AIA-09-2018-0036
Attanasio, M., Masedu, F., Quattrini, F., Pino, M. C., Vagnetti, R., Valenti, M., & Mazza, M. (2022). Are Autism Spectrum Disorder and Asexuality Connected?. Archives of sexual behavior, 51(4), 2091–2115. https://doi.org/10.1007/s10508-021-02177-4 Bowman, S. J., Casey, L. J., McAloon, J., & Wootton, B. M. (2022). Assessing gender dysphoria: A systematic review of patient-reported outcome measures. Psychology of Sexual Orientation and Gender Diversity, 9(4), 398–409. https://doi.org/10.1037/sgd0000486 Cooper, K., Mandy, W., Butler, C., & Russell, A. (2022). The lived experience of gender dysphoria in autistic adults: An interpretative phenomenological analysis. Autism, 26(4), 963-974. https://doi-org.csu.idm.oclc.org/10.1177/13623613211039113 Davies, C., Moosa, M., McKenna, K., Mittal, J., Memis, I., Mittal, R., & Eshraghi, A. A. (2023). Quality of Life, Neurosensory Disorders and Co-Occurring Medical Conditions in Individuals on the Spectrum, with a Special Focus on Females Diagnosed with Autism: A Systematic Review. Journal of clinical medicine, 12(3), 927. https://doi.org/10.3390/jcm12030927 Ehrensaft, D. (2018). Double Helix Rainbow Kids. Journal of Autism and Developmental Disorders, 48(12), 4079-4081. https://doi-org.csu.idm.oclc.org/10.1007/s10803-018-3716-5 Gasser, B. A., Buerki, S. F., Kurz, J., & Mohaupt, M. G. (2021). Hyperandrogenism? Increased 17, 20-Lyase Activity? A Metanalysis and Systematic Review of Altered Androgens in Boys and Girls with Autism. International journal of molecular sciences, 22(22), 12324. https://doi.org/10.3390/ijms222212324 Gasser, B., Kurz, J., Escher, G., Mistry, H. D., & Mohaupt, M. G. (2022). Androgens Tend to Be Higher, but What about Altered Progesterone Metabolites in Boys and Girls with Autism?. Life (Basel, Switzerland), 12(7), 1004. https://doi.org/10.3390/life12071004 George, R., & Stokes, M. A. (2018). Gender identity and sexual orientation in autism spectrum disorder. Autism : the international journal of research and practice, 22(8), 970–982. https://doi.org/10.1177/1362361317714587 Gomes, S. M., Jacob, M. C., Rocha, C., Medeiros, M. F., Lyra, C. O., & Noro, L. R. (2021). Expanding the limits of sex: a systematic review concerning food and nutrition in transgender populations. Public health nutrition, 24(18), 6436–6449. https://doi.org/10.1017/S1368980021001671 Heylens, G., Aspeslagh, L., Dierickx, J., Baetens, K., Van Hoorde, B., De Cuypere, G., & Elaut, E. (2018). The Co-occurrence of Gender Dysphoria and Autism Spectrum Disorder in Adults: An Analysis of Cross-Sectional and Clinical Chart Data. Journal of autism and developmental disorders, 48(6), 2217–2223. https://doi.org/10.1007/s10803-018-3480-6 Holt, N. R., Ralston, A. L., Hope, D. A., Mocarski, R., & Woodruff, N. (2021). A systematic review of recommendations for behavioral health services for transgender and gender diverse adults: The three-legged stool of evidence-based practice is unbalanced. Clinical Psychology: Science and Practice, 28(2), 186–201. https://doi-org.csu.idm.oclc.org/10.1037/cps0000006.supp (Supplemental) Jones, R. M., Wheelwright, S., Farrell, K., Martin, E., Green, R., Di Ceglie, D., & Baron-Cohen, S. (2012). Brief report: female-to-male transsexual people and autistic traits. Journal of autism and developmental disorders, 42(2), 301–306. https://doi.org/10.1007/s10803-011-1227-8 Kallitsounaki, A., & Williams, D. M. (2023). Autism Spectrum Disorder and Gender Dysphoria/Incongruence. A systematic Literature Review and Meta-Analysis. Journal of Autism & Developmental Disorders, 53(8), 3103–3117. https://doi-org.csu.idm.oclc.org/10.1007/s10803-022-05517-y Kirkovski, M., Enticott, P. G., & Fitzgerald, P. B. (2013). A review of the role of female gender in autism spectrum disorders. Journal of autism and developmental disorders, 43(11), 2584–2603. https://doi.org/10.1007/s10803-013-1811-1 Libsack, E. J., Keenan, E. G., Freden, C. E., Mirmina, J., Iskhakov, N., Krishnathasan, D., & Lerner, M. D. (2021). A Systematic Review of Passing as Non-autistic in Autism Spectrum Disorder. Clinical child and family psychology review, 24(4), 783–812. https://doi.org/10.1007/s10567-021-00365-1 Lim, M., Carollo, A., Dimitriou, D., & Esposito, G. (2022). Recent Developments in Autism Genetic Research: A Scientometric Review from 2018 to 2022. Genes, 13(9), 1646. https://doi.org/10.3390/genes13091646 Maroney, M. R., & Horne, S. G. (2022). “Tuned into a different channel”: Autistic transgender adults’ experiences of intersectional stigma. Journal of Counseling Psychology, 69(6), 761–774. McKenna, B. G., Huang, Y., Vervier, K., Hofammann, D., Cafferata, M., Al-Momani, S., … Michaelson, J. J. (2021). Genetic and morphological estimates of androgen exposure predict social deficits in multiple neurodevelopmental disorder cohorts. Molecular Autism, 12, 1-18. doi:http://dx.doi.org/10.1186/s13229-021-00450-w Mezzalira, S., Scandurra, C., Mezza, F., Miscioscia, M., Innamorati, M., & Bochicchio, V. (2022). Gender Felt Pressure, Affective Domains, and Mental Health Outcomes among Transgender and Gender Diverse (TGD) Children and Adolescents: A Systematic Review with Developmental and Clinical Implications. International journal of environmental research and public health, 20(1), 785. https://doi.org/10.3390/ijerph20010785 Nobili, A., Glazebrook, C., Bouman, W. P., Glidden, D., Baron-Cohen, S., Allison, C., Smith, P., & Arcelus, J. (2018). Autistic Traits in Treatment-Seeking Transgender Adults. Journal of Autism & Developmental Disorders, 48(12), 3984–3994. https://doi-org.csu.idm.oclc.org/10.1007/s10803-018-3557-2 Pinna, F., Paribello, P., Somaini, G., Corona, A., Ventriglio, A., Corrias, C., Frau, I., Murgia, R., El Kacemi, S., Galeazzi, G. M., Mirandola, M., Amaddeo, F., Crapanzano, A., Converti, M., Piras, P., Suprani, F., Manchia, M., Fiorillo, A., Carpiniello, B., & Italian Working Group on LGBTQI Mental Health (2022). Mental health in transgender individuals: a systematic review. International review of psychiatry (Abingdon, England), 34(3-4), 292–359. https://doi.org/10.1080/09540261.2022.2093629 Rojas Saffie, J. P., & Eyzaguirre Bäuerle, N. (2023). Etiology of gender incongruence and its levels of evidence: A scoping review protocol. PloS one, 18(3), e0283011. https://doi.org/10.1371/journal.pone.0283011 Shah, D., Bobade, S. (2018). Polycystic Ovarian Syndrome and Autism. Journal of Psychosocial Research; New Delhi 13(2), 435-442. DOI:10.32381/JPR.2018.13.02.18 Strang, J. F., Kenworthy, L., Dominska, A., Sokoloff, J., Kenealy, L. E., Berl, M., Walsh, K., Menvielle, E., Slesaransky-Poe, G., Kim, K. E., Luong-Tran, C., Meagher, H., & Wallace, G. L. (2014). Increased gender variance in autism spectrum disorders and attention deficit hyperactivity disorder. Archives of sexual behavior, 43(8), 1525–1533. https://doi.org/10.1007/s10508-014-0285-3 Strang, J. F., Knauss, M., van der Miesen, A., McGuire, J. K., Kenworthy, L., Caplan, R., Freeman, A., Sadikova, E., Zaks, Z., Pervez, N., Balleur, A., Rowlands, D. W., Sibarium, E., Willing, L., McCool, M. A., Ehrbar, R. D., Wyss, S. E., Wimms, H., Tobing, J., Thomas, J., … Anthony, L. G. (2021). A Clinical Program for Transgender and Gender-Diverse Neurodiverse/Autistic Adolescents Developed through Community-Based Participatory Design. Journal of clinical child and adolescent psychology : the official journal for the Society of Clinical Child and Adolescent Psychology, American Psychological Association, Division 53, 50(6), 730–745. https://doi.org/10.1080/15374416.2020.1731817 Strang, J. F., Wallace, G. L., Michaelson, J. J., Fischbach, A. L., Thomas, T. R., Jack, A., Shen, J., Chen, D., Freeman, A., Knauss, M., Corbett, B. A., Kenworthy, L., Tishelman, A. C., Willing, L., McQuaid, G. A., Nelson, E. E., Toomey, R. B., McGuire, J. K., Fish, J. N., Leibowitz, S. F., … Yang, J. S. (2023). The Gender Self-Report: A multidimensional gender characterization tool for gender-diverse and cisgender youth and adults. The American psychologist, 78(7), 886–900. https://doi.org/10.1037/amp0001117 Tankersley, A. P., Grafsky, E. L., Dike, J., & Jones, R. T. (2021). Risk and Resilience Factors for Mental Health among Transgender and Gender Nonconforming (TGNC) Youth: A Systematic Review. Clinical child and family psychology review, 24(2), 183–206. https://doi.org/10.1007/s10567-021-00344-6 Thrower, E., Bretherton, I., Pang, K. C., Zajac, J. D., & Cheung, A. S. (2020). Prevalence of Autism Spectrum Disorder and Attention-Deficit Hyperactivity Disorder Amongst Individuals with Gender Dysphoria: A Systematic Review. Journal of autism and developmental disorders, 50(3), 695–706. https://doi.org/10.1007/s10803-019-04298-1 Walker, M. (2021). Exploring The Cyc Cis-Tem: A Literature Review Of Queer And Trans Topics In Child And Youth Care. International Journal of Child, Youth and Family Studies 12(3-4), 23–54. https://doi.org/10.18357/ijcyfs123-4202120333
0 Comments
 What is Neurodiversity, Anyway?by Lisa Macafe Just as the word queer encompasses a variety of identities under the LGBTQ+ umbrella, the word neurodiversity also encompasses spectrums of differences and society has seemingly deemed both groups inferior to the able-bodied, neurotypical, cisgender, heterosexual person, which causes people in marginalized identities challenges (Kafer, 2009; Legault et al., 2021). Neurodiversity consists of various natural divergences in neurological function such as autism, attention deficit hyperactivity disorder (ADHD), Tourette’s, or dyslexia, and was first coined by Judy Singer in the 1990s, who used the term to refer only to autistic people (Doyle & McDowall, 2022; Fung et al., 2022; Goldberg, 2023; Legault et al., 2021). Neurodivergent people are any whose neurology deviates from the typical cognitive profile normed by society. Neurotypical people are those whose neurology matches the accepted norm (Fletcher-Watson, 2022; Legault et al., 2021). Neuro-minorities may be developmental, such as autism and ADHD, or acquired, such as depression or amnesia (Goldberg, 2023). 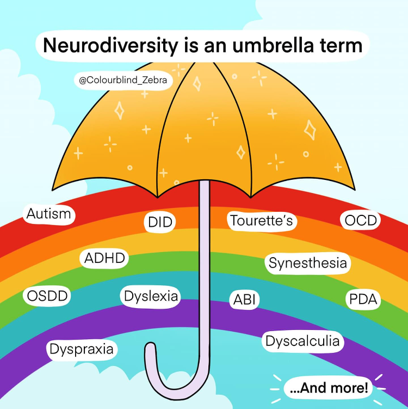 There are many characteristics in common between different neurodivergent identities including information processing similarities, similar experiences, and atypical responses to stimuli (Fletcher-Watson, 2022). Neurodiversity could apply to anyone whose brain function is atypical, about 20% of humanity, including people with schizophrenia, bipolar disorder, and major depressive disorders, but consensus has not been reached on how broadly to apply the neurodivergent label and most people consider neurodiversity to refer to neurodevelopmental conditions and not mental health identities (Doyle & McDowall, 2022; Goldberg, 2023). 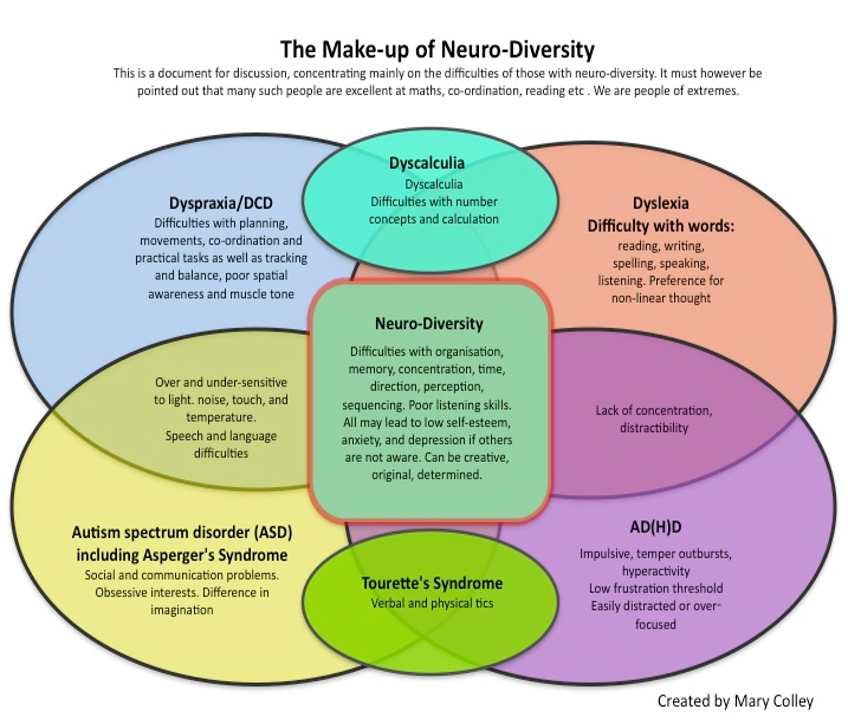 Neurodiversity theory draws on the ideas of crip theory, created by Robert McRuer in the early 2000s, that was made to deconstruct ideas about disability and being disabled and focuses on how reality can be re-shaped and re-imagined to allow for other ways of being to exist. It avoids use of the word “normal” in favor of modalities allowing individuals to, not just survive, but flourish, while existing outside of assimilation and typicality (Kafer, 2009). Crip theory rejects ableism (Abrams & Abes, 2021). Ableism is a kind of compulsory able-mindedness and able-bodiedness valuing bodies and minds that are typical above the atypical, giving them space in the world (Kafer, 2009). Disability is, however, a naturally occurring variation in humans, and all people are normal – although not all people are typical (Abrams & Abes, 2021). The neurodiversity paradigm states neurodevelopmental conditions such as autism are simple and natural biological differences similar to sexual orientation or skin color and are not in need of being changed (Goldberg, 2023; Legault et al., 2021; Lerner et al, 2023; Shields & Beversdorf, 2021). Biological diversity is naturally occurring and supports the overall health of the species. Being atypical is not problematic for evolution, atypicality is a natural distribution of cognitive function across the species just like being very tall (Goldberg, 2023). Neuro-minorities fall within the normal distribution of human experience and are not abnormal (Doyle & McDowall, 2022; Fletcher-Watson, 2022). Neurodivergence in general is beneficial to society by increasing genetic variation, flexibility, and evolvability (Goldberg, 2023). For people who are disabled and queer, assimilationist ideologies will never work to build authentic paradigms of power and privilege, because the individual will always be fundamentally different from what is expected as typical. Essentially, crip theory argues that while queer disabled people are constantly being displaced by society, the brightest possibilities come about in the refusal of displacement (Kafer, 2009). For many neurodivergent folks, sex, gender, and sexuality are performative acts based on the internalization of societal expectations and the individual’s situation. Sexual orientation and gender identity also change over time and are not pre-determined (Verma et al., 2023). Queer theory resists normalizing and privileging certain identities over others and encourages society to resist policing other people’s expressions outside of the commonly accepted binary identities (Verma et al., 2023). Autistic people do not all fit conveniently into the gender binaries of male and female and some break down the heteronormative structures and pressure to conform, question assumptions about gender and sexuality, focus on the systems of power that divide, and support people who identify as transgender or non-binary (Carroll & Gilroy, 2001). Transgender people are often given more privilege and power in society if they perform a cisgender role, but this may feel inauthentic to their true self and prevent them having genuine relationships for fear of being “found out”. Conversely, adopting a queer identity as a transgender person risks danger and abuse in the world; attaining a state of good mental health may be very difficult for some without the rejection of the binary and safe living situations (Jones, 2021). Queer and transgender people simply existing disrupt systems of power that contribute to others living artificially or stigmatizing roles due to fear and aid others in questioning their assumptions on gender and sexuality (Jones, 2021).  Neurodiversity theory has been a political rallying cry to encourage individuals to think outside the neurotypical boxes society has construed as the only options and has encouraged people to create new ways of being that do not involve being stuck inside of binary socially prescribed attitudes and beliefs (Legault et al., 2021). It is important when individuals realize the neurotypical roles they have internalized become restrictive or harmful, they leave internalized ableist ideas behind to forge a future that affirms their neurodiversity (Schuck, 2023). Many autistic queer people critically evaluate schemas purported to be “normal” (such as gender roles) to identify harmful elements perpetuated in order to keep certain populations in power and others minoritized (Kokkos, 2022). Autism treatment in the past built on the medical model of disability wherein autism was viewed from a disorder framework as something that could be fixed. Treatment was often geared towards the individual learning to mimic typical behaviors, often at great cost to self (Schuck, 2023). The neurodiversity movement diverged from the medical (deficit) model of disability, stating autistic people do not need to be typical or fixed to have worth and autistic people deserve to be accepted and included in society as they are (Butler, 2023; Goldberg, 2023). If society pressures individuals to conform to mainstream norms, is often harmful to the individual. The neurodiversity paradigm builds on the social model of disability that says autistic people are disabled not by an inherent flaw within themselves, rather society is disabling to autistic people by not accommodating their needs (Enoka, 2022; Goldberg, 2023). Instead of asking how the autistic person can be made to fit into typical society, the neurodiversity movement asks how society can build affirming environments and embed supports so neurodivergent people can thrive and not just survive (Butler, 2023; Fung et al., 2022; Legault et al., 2021). 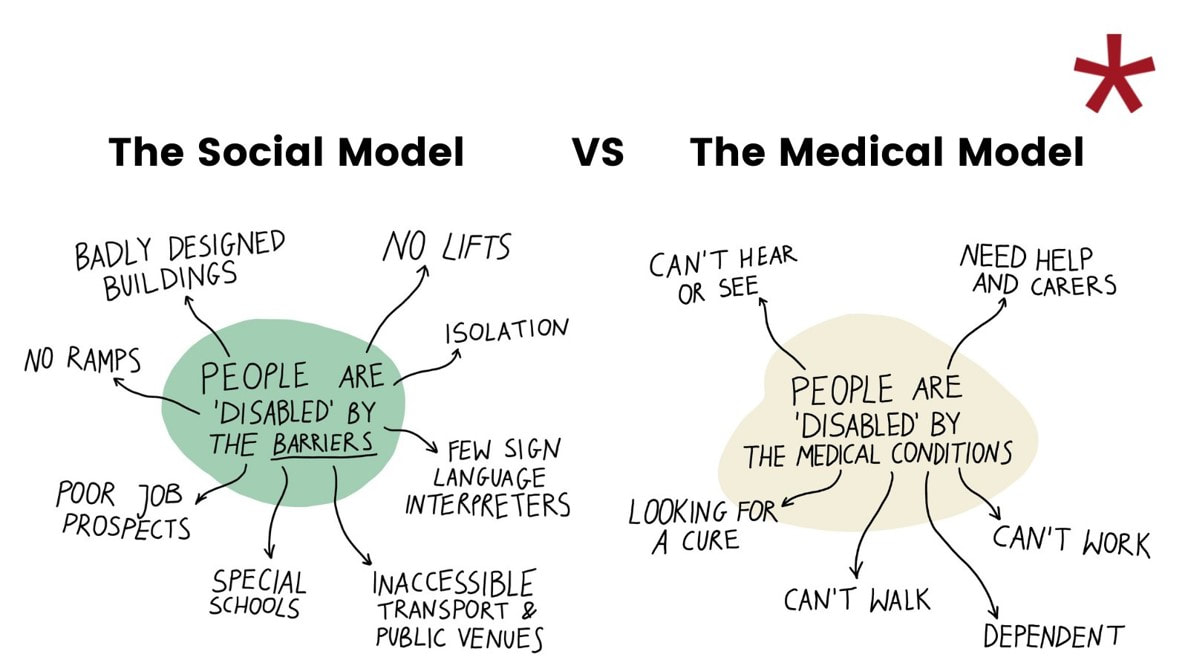 The neurodiversity paradigm ascribes to recognizing the lived experiences and self-diagnosis of neurodivergent people as comparable to clinical experts’ thoughts on neurodiversity (Fletcher-Watson, 2022). Historically, voices of parents of autistic children and non-autistic researchers have been uplifted while voices of autistic people themselves have been silenced. Neurotribes laid foundations for a historical approach to neurodiversity by tracing the history of neurodiversity from the simultaneous first research on autistic children by Hans Asperger and Leo Kanner’s research in the 1940s, the refrigerator mother theory that cold mothers created autistic children in the 1950s, Ivar Lovaas creating ABA to train autistic children in the 1970s, and through to modern figures and discussions on neurodiversity today (Silberman, 2015). The neurodiversity movement seeks to improve societal support towards inclusion instead of correction (Goldberg, 2023). Neurodivergent people have been discriminated against for not being neurotypical, when they had no control over being born into the neuro-minority (Curnow et al., 2023; Fung et al., 2022; Goldberg, 2023; Legault et al., 2021). Continuing to address autism as solely an absence of neurotypical behavior neglects the strengths autistic people have and may de-focus accommodations that enable wellbeing (Fung et al., 2022; Shields & Beversdorf, 2021). Support should be designed around non-judgmental identification and acceptance of unmet needs and neurodivergent-affirming accommodations to meet those needs, such as fidget toys, movement breaks, or noise cancelling headphones allowed during school or at work (Fletcher-Watson, 2022). Simple shifts in expectations can allow neuro-minorities to become valuable team members and live more meaningful lives (Doyle & McDowall, 2022). There are controversies discussing the way autistic people should be supported (Schuck, 2023). Interventions for autistic people not taking autistic perspectives into account when designing goals have been found to be harmful to overall mental health (Butler, 2023; Enoka, 2022; Lerner et al, 2023). Some treatment outcomes for autistic children, especially from ABA, emphasize compliance with parent desires and suppression of autistic behaviors, such as stimming, to be replaced with neurotypical behaviors, such as eye contact (Curnow et al., 2023). If the goal of treatment is erasure of self, compliance, and normalization, problems in mental health will result (Legault et al., 2021). The higher rates of anxiety and depression that autistic people experience fuel the neurodiversity movement’s push to change the services provided (Butler, 2023). The Autistic Self Advocacy Network (ASAN) adopted its slogan, ‘nothing about us, without us,’ to petition the public to allow autistic people a say in the services and policies affecting them (Enoka, 2022; Legault et al., 2021).  Autism experts are autistic people. Those purporting to be experts on autism who are neurotypical must collaborate with autistic people to get an informed perspective on their work (Enoka, 2022). For optimal ethical results, treatment goals should incorporate the perspective of the individual receiving treatment (Curnow et al., 2023; Lerner et al, 2023) and the autistic person should validate the treatment they are receiving and give feedback for future work. Professionals in the autism field should assess their attitude towards neurodiversity (Schuck, 2023). Autistic adults’ input can be instrumental in designing future practices and determine if interventions may be more harmful than helpful (Curnow et al., 2023). The neurodiversity movement advocates for rights and removing the pathologizing of autism and other diagnosis (Shields & Beversdorf, 2021). Neurotypical people both are the norm and create and enforce the norms autistic people are judged by (Legault et al., 2021). Some underappreciated traits common in autistic people are the tendency not to lie and to be highly ethical, tendency to work hard and be impassioned about their interests, sustaining long work hours related to their passions, having deep empathy, caring for the wellbeing of others (even those they do not know), and explaining their thoughts directly without euphemism or decoding needed (Enoka, 2022; Fung et al., 2022). "Autism awareness" is a problematic term because autism is not a disease to be caught or cured, it is a neurodevelopmental condition that is a biological difference in the brain (Legault et al., 2021; Schuck, 2023). Jim Sinclair led the autism rights movement and pushed people to accept variation instead of trying to "cure" autistic children (Fung et al., 2022). To imply to parents that children can be ‘cured’ implies treatments can change the neurology of their brain, which is false, and implies autistic people are not good enough the way they are and need to be fixed, which is damaging (Schuck, 2023). Having a positive identity based on strengths and interests instead of a deficit mentality about the lack of neurotypicality can help neurodivergent people embrace their unique skills. When autistic minds are allowed to flourish, it opens the world to the possibility of groundbreaking outside the box thinking from people such as past autistics like Alan Turning and Albert Einstein (Fung et al., 2022). To summarize, the neurodiversity movement pushes to have autism and other forms of neurodivergence such as ADHD, epilepsy, and learning disabilities de-pathologized and move from the medical model of disability that places the onus of change on the disabled individual, to the social model of disability where individuals are disabled by the society not providing access or accommodations so that they can live their most full and happy lives (Enoka, 2022). The neurodiversity framework seeks to normalize difference as natural and see difference as a strength that allows for innovation, not just as a deficit because they are not matching to typical norms and expectations (Legault et al., 2021). 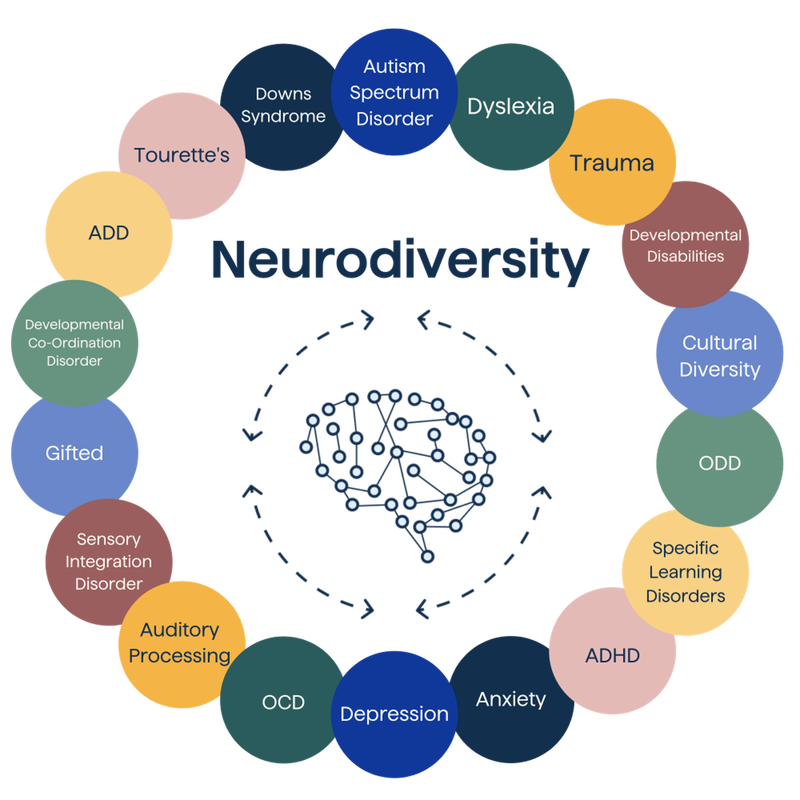 References
Abrams, E. J., & Abes, E. S. (2021). "It's Finding Peace in My Body": Crip Theory to Understand Authenticity for a Queer, Disabled College Student. Journal of College Student Development, 62(3), 261-275. http://proxy1.calsouthern.edu/login?url=https://www-proquest-com.csu.idm.oclc.org/scholarly-journals/finding-peace-my-body-crip-theory-understand/docview/2547639324/se-2 Butler, S. (2023). A Narrative Inquiry Into the Neurodivergent Identity (Order No. 30568592). Available from ProQuest One Academic. (2833872272). https://csu.idm.oclc.org/login?url=https://www-proquest-com.csu.idm.oclc.org/dissertations-theses/narrative-inquiry-into-neurodivergent-identity/docview/2833872272/se-2 Carroll, L., & Gilroy, P. J. (2001). Teaching “Outside the Box”: Incorporating Queer Theory in Counselor Education. Journal of Humanistic Counseling, Education & Development, 40(1), 49–58. https://doi-org.csu.idm.oclc.org/10.1002/j.2164-490X.2001.tb00101.x Carroll, S. (2019). Respecting and empowering vulnerable populations: Contemporary terminology. The Journal for Nurse Practitioners, 15(3), 228-231. https://doi-org.csu.idm.oclc.org/10.1016/j.nurpra.2018.12.031 Creswell, J. D. & Cresswell, J. W. (2018). Research design: Qualitative, quantitative, and mixed methods approaches. (5th ed.). Sage. Curnow, E., Rutherford, M., Maciver, D., Johnston, L., Prior, S., Boilson, M., Shah, P., Jenkins, N., & Meff, T. (2023). Mental health in autistic adults: A rapid review of prevalence of psychiatric disorders and umbrella review of the effectiveness of interventions within a neurodiversity informed perspective. PLoS One, 18(7)https://doi-org.csu.idm.oclc.org/10.1371/journal.pone.0288275 Doyle, N., & McDowall, A. (2022). Diamond in the rough? An “empty review” of research into “neurodiversity” and a road map for developing the inclusion agenda. Equality, Diversity and Inclusion: An International Journal, 41(3), 352-382. https://doi-org.csu.idm.oclc.org/10.1108/EDI-06-2020-0172 Enoka, K. (2022). An Early Career Music Therapist's Reflections on the Neurodiversity Paradigm and Implications for Advocating for Neurodivergent Participants through Reporting for NDIS: Small Steps in an Agonistic Journey. The Australian Journal of Music Therapy, 33(2), 37-46. https://csu.idm.oclc.org/login?url=https://www-proquest-com.csu.idm.oclc.org/scholarly-journals/early-career-music-therapists-reflections-on/docview/2782965487/se-2 Fletcher-Watson, S. (2022). Transdiagnostic research and the neurodiversity paradigm: commentary on the transdiagnostic revolution in neurodevelopmental disorders by Astle et al. Journal of Child Psychology & Psychiatry, 63(4), 418–420. https://doi-org.csu.idm.oclc.org/10.1111/jcpp.13589 Fung, L. K., Ulrich, T. L., Fujimoto, K. T., & Taheri, M. (2022). NEURODIVERSITY: AN INVISIBLE STRENGTH? Jom, 74(9), 3200-3202. https://doi-org.csu.idm.oclc.org/10.1007/s11837-022-05454-2 Goldberg, H. (2023). Unraveling Neurodiversity: Insights from Neuroscientific Perspectives. Encyclopedia, 3(3), 972. https://doi-org.csu.idm.oclc.org/10.3390/encyclopedia3030070 Hall, J. P., Katie, B., Streed, C. G., Jr, Boyd, B. A., & Kurth, N. K. (2020). Health disparities among sexual and gender minorities with autism spectrum disorder. Journal of Autism and Developmental Disorders, 50(8), 3071-3077. https://doi-org.csu.idm.oclc.org/10.1007/s10803-020-04399-2 Jones, R. M., Wheelwright, S., Farrell, K., Martin, E., Green, R., Di Ceglie, D., & Baron-Cohen, S. (2012). Brief report: female-to-male transsexual people and autistic traits. Journal of autism and developmental disorders, 42(2), 301–306. https://doi.org/10.1007/s10803-011-1227-8 Kafer, A. (2009). What's Crip About Queer Theory Now?: Crip Theory: Cultural Signs of Queerness and Disability. By Robert McRuer, New York, New York University Press, 2006. 283 pp. Sex Roles, 60(3-4), 291-294. https://doi-org.csu.idm.oclc.org/10.1007/s11199-008-9511-6 Kokkos, A. (2022). Transformation theory as a framework for understanding transformative learning. Adult Education – Critical Issues (2)2, 20-33. Retrieved from https://www.researchgate.net/publication/366826194_Transformation_Theory_as_a_Framework_for_Understanding_Transformative_Learning on May 31st 2023. Legault, M., Bourdon, J., & Poirier, P. (2021). From neurodiversity to neurodivergence: the role of epistemic and cognitive marginalization. Synthese, 199(5-6), 12843-12868. https://doi-org.csu.idm.oclc.org/10.1007/s11229-021-03356-5 Schuck, R. K. (2023). Moving Toward Neurodiversity-Affirming Services for Autistic Individuals: Social Validity, Autistic Perspectives, and Measuring Attitudes (Order No. 30527731). Available from ProQuest One Academic. (2859578983). https://csu.idm.oclc.org/login?url=https://www-proquest-com.csu.idm.oclc.org/dissertations-theses/moving-toward-neurodiversity-affirming-services/docview/2859578983/se-2 Shields, K., & Beversdorf, D. (2021). A dilemma for neurodiversity. Neuroethics, 14(2), 125–141. https://doi.org/10.1007/s12152-020-09431-x Silberman, S. (2015). Neurotribes: the legacy of autism and the future of neurodiversity. New York, Avery, an imprint of Penguin Random House. Verma, T., Chapman-Orr, E., Davis, A. What is queer theory? Grinnell College: Subcultures and Society. Retrieved from https://haenfler.sites.grinnell.edu/subcultural-theory-and-theorists/queer-theory/ on May 31st, 2023. A Slow DeclinEby Lisa Macafe I wrote A Slow Decline to describe what living with chronic fatigue syndrome/ myalgic encephalomyelitis (CFS/ME) is like and how chronic health conditions like this are related to autism.  I have had health issues all my life, but they were always things that could be dealt with.
My first brush with the ER (that I remember) was when I was eight years old and got a migraine that no one could stop. I remember crying and everything being terrible. I continued to get migraines regularly until a few years ago when the monthly preventative injection drugs came out (hallelujah!) and now I only get a few a month. My next foray into medical quandaries was at 16 when I had a ruptured ovarian cyst from PCOS that put me in the hospital at the same time as my dad, who had appendicitis - woo-hoo for family bonding! They had to run a whole lot of tests to figure out what was going on with me, because, apparently, my organs are not in the typical place and they couldn’t find my ovaries. Fun. The cysts still require medication to stop from exploding. Over the years, I have collected more health issues, as many people do. In addition to PCOS and migraines, I added hypoglycemia, scoliosis, hypothyroidism, fibromyalgia, joint hypermobility, autism, anxiety, depression, and TMJD. These have all been manageable with lifestyle, therapy, and medication. I think something happened in the last few years though. My theory is that I have lived most of my life in a near constant state of hyper-vigilance due to fear and anxiety. I have always been autistic, but did not know it until age 37, and always felt “off” from other people. I was isolated, even with other people, and felt like a fraud. I worked very hard as an adult to match how I appeared with what I thought was expected. I kept myself thin, dressed in boring “normal” clothes, kept my hair and makeup “nice”. I patrolled the words coming out of my mouth in fear that my thoughts might disquiet others. I monitored the way my body moved to stop myself from self-stimulating behavior that calmed me but looked “weird” and made people uncomfortable. And I still terrified all the time. No amount of precautions were enough. I still don’t know what I was scared of, but the fear was visceral and real. Aching fear pervading my life is the main reason I fell so hard into substance use as a young person. The only way to escape the clutching anxiety about everything was to force my brain to slow down using substances. I could get no respite without their help. Once I had children, everything changed. No more partying, no more erasing myself with forced conformity. I couldn’t do it anymore. I was too tired, and kids gave me a confidence that I never had before - a feeling that I mattered and deserved a place in this world so that I could look after my babies and create space for them to be happy. We have to lead by example, and I wanted to be a good example for them on living as themselves. I am loud about being autistic, dyed my hair pink, and have stopped trying to impress other people so much. It never seemed to work anyways, they seemed to just sense something was “off” about me and assumed nasty things about what it was. So here I am. Living as authentically as I am able, advocating for others like me, and in a career that I genuinely love (and finally in a full-time position, too)! So why is my health failing worse than ever? As far as I can tell, living from age 10 to 37 under chronic stress and fear does damage. It turns out, I cannot continue to “just power through” when I get tired. I need to rest, and now, if I don’t, my body will force a shut down. Enter chronic fatigue syndrome/ myalgic encephalomyelitis (CFS/ME). My newest diagnosis and the worst by far. It sounds so innocent - “we all get a little tired every now and then”, right? But this is some crazy effect. I’m too tired to sit up sometimes now. Too tired to operate the electric mobility scooter we bought. Too tired to find words to express what I need. And then I’ll rest for a while and feel better and forget that I have this thing. I’ll live pretty normally and do just slightly too much and I’m back to feeling decrepit again for a week or so. The doctors don’t have any treatments that will improve things, the recommendation is to rest. So I live in this cycle of trying to stay in the margins of my energy envelope, but the margins keep unremittingly shrinking as this thing persists. I used to hike for hours. Fence. Play tennis. Now I can’t even chase my kids on the playground or play competitive video games. So many things are lost to me. I am trying to think where I can take my kids on vacation this summer that I would be able to enjoy… and I’m fresh out of ideas. It seems like each year I can do a little bit less. I am hopeful to be able to find a root cause and be able to treat it, but fear my reality is now the slow decline that has permeated my life of late. And yet, I still feel like myself. I still dream and ponder life’s mysteries. My doctorate program has been a fantastic outlet for me to apply my mind to problems that don’t require a physical solution. I persist. Trans Day of Remembrance Monday November 20 Hello friends, November 20th is Trans Day of Remembrance, a time to look back and remember those we have lost, give our respects, and look forward with renewed determination. Anti-trans violence is prolific. In the last year there have been more than 320 murders of trans people, with highest rates in Brazil (107), the United States (62), Mexico (52), and Columbia (21) [map]. To see some of their stories, click here. More than 4,600 trans / non-binary people having been murdered since 2008 when Trans Respect first began tracking. Remembering Our Dead - Reports index tdor.translivesmatter.info Internalized transphobia, lack of acceptance, and chronic fear contribute to adverse mental health outcomes for the trans community. In addition to murder, suicide claims a large number of us. According to the Williams Institute, 81% of trans adults have thought about suicide, 42% have attempted, and others engage in risky behaviors such as self-harm and substance use. All that being said, we can each make a difference. Access to gender affirming care, which can be as simple as respecting chosen names, pronouns, and clothing choices, can reduce suicide risks by 73%, and just one gender affirming adult in a person's life can be the difference needed to prevent suicide. Suicide Risk Reduces 73% in Transgender, Nonbinary Youths with Gender-Affirming Care Transgender and nonbinary youths, a population with an exceptional risk of suicide and poor mental health outcomes, were found to have 60% lower odds of depression after receiving gender-affirming intervention. www.hcplive.com "Transgender people face extraordinary levels of physical and sexual violence, whether on the streets, at school or work, at home, or at the hands of government officials. More than one in four trans people has faced a bias-driven assault, and rates are higher for trans women and trans people of color... This effort cannot be limited to just Transgender Day of Remembrance. Public education, policy change and community efforts are needed to address the complex causes of anti-trans violence and ensure victims can receive support." - TransEquality.org We can all make the world a little bit better by showing up, speaking out for, and uplifting trans and non-binary people. I invite you to join me for an informal Trans Day of Remembrance event Monday November 20th in JSC-101 The Spot from 12pm-1pm to talk, share stories, express anxieties, or ask questions. I hope to see you there!  Evidence-Based Treatments For Autistic Adultsby Lisa Macafee Autistic gender diverse people may need different treatments than the typical population because their neurology is different from a neurotypical person’s. Queer autistic people experience disproportionate rates of mental and physical health troubles, including anxiety, depression, obsessive compulsive disorder, substance use disorder, increased smoking, early death, and other health conditions (Hall, et al., 2021). There is no established pharmacological treatment for autism (Aran et al., 2021) and traditional treatments can be difficult for autistic people due to challenges with sensory sensitivities, executive functioning, difficulty with theory of mind, identifying and managing emotions and feelings, and cognitive flexibility that many treatments rely on (Spain et al., 2020). Treatments such as group therapy, for example, may be especially unhelpful for autistic adults due to the pressures of social anxiety and personalized intervention plans are often needed (Helverschou et al., 2019). Evidence Based Treatment for Autistic Adults General Recommendations Autistic people face complex challenges when accessing health care, but there are some practical and simple strategies that providers can implement to make their practices more accessible. Doherty et al. (2022) state that challenges most common for autistic people are stressors involved in communication such as making appointments on the phone, being misunderstood or not listened to, not being able to follow along with what the providers is saying, sensory challenges in waiting rooms and offices, and lack of predictability for cancellations or wait times. Adjustments for autistic people can be implemented by providers understanding how autism impacts people and offering simple changes such as multiple modalities for scheduling appointments instead of requiring a phone call (Doherty et al., 2022). Mayor (2021) found that simple strategies adopted by health care providers can make significant differences in autistic people’s anxiety levels when seeking treatment. Phrasing questions in clear and concise language that cannot be misinterpreted, offering a quiet waiting space for appointments, seeing appointments on time, minimizing cancellations, and exhibiting patience, calm, and respect for clients makes seeking services much less anxiety-producing for autistic people (Mayor, 2021). Some of the best evidence based practices for autistic people can be learning about how autistic people function and finding basic techniques to reduce stress and maximize wellbeing. Ghanouni & Quirke (2023) found coping strategies that can be most effective for autistic people are engaging in their special interests, recreational and leisure activities, taking regular breaks for sensory and emotional regulation, regular socialization, and having supportive relationships. They state two generalized strategies useful for autistic people are problem-focused coping and emotion-focused coping where the individual focuses on mitigating negative emotions and attribute meaning to stressful situations. Especially noted as helpful for autistic adults were technology supports such as phone alarms and checklist apps that allow tracking of required daily tasks, but also technology used for social connection and networking. Technology supports help autistic people address needs without triggering social anxiety and timed social responses that can cause so much stress. Learning how autism affects individuals so they can understand and better moderate their challenges, understand their own strengths and weaknesses, learn more about other autistic people, and how the individual’s challenges are common or unique are beneficial to autistic overall wellbeing (Ghanouni & Quirke, 2023). Some simple strategies recommended by autistic AFAB people are to take time for oneself to prevent burnout, creating supportive routines and structure, and un-learning the tendency to mask all autistic behaviors as this often leads to increased stressors, and for some, loss of sense of self (Miner, et. all, 2019). Maladaptive coping strategies such as avoidance, self-blame, and masking should be avoided as they can lead to autistic burnout, a focus of intervention should be on leaning into healthy coping strategies and de-focusing unhealthy coping strategies (Ghanouni & Quirke, 2023). While autism is a marked by challenges in social function, that does not mean that socialization is not important for autistic people. Social inclusion, supportive social relationships, and feeling belonging can be helpful to increase resilience among autistic individuals (Ghanouni & Quirke, 2023). According to Djela (2021), one large impact to increase social inclusion, belonging, and increased social support for autistic people is finding productive employment. They state 77% of autistic adults are unemployed but want to work and only 16% work full-time. Autistic people are often undervalued and discriminated against in the workforce due to stigma and fear and having atypical behavioral or social responses, but often have underappreciated skills of work ethic, methodical approach to tasks, reliability, innovative thinking, and in-depth interest in topics (Djela, 2021). Autistic people can be productive employees that are true assets to their workplace with a few basic accommodations. Accommodations in the workplace such as not requiring social masking where the autistic person tries to appear typical, allowing noise cancelling earbuds, being able to take sensory breaks, and other steps can help autistic adults thrive at work and allow for more social engagement (Djela, 2021). Social engagement for autistic people can be just as important to mental health as for neurotypical people, there are simple challenges to be worked through for autistic people to do so. Cognitive Behavioral Therapy Adapted cognitive behavioral therapy (CBT) has been found to be especially effective for autistic adults. Autistic people using CBT therapies were found to have significant improvements in depression, anxiety, stress, social anxiety, fear, avoidance, and restricted and repetitive behaviors, and increase social motivation, and overall mental health (Bemmer et al., 2021). CBT is a goal-based form of talking therapy based on understanding the relationships between thoughts, feelings, and actions, identifying unhealthy thought patterns and developing effective coping strategies to stop harmful thought cycles, and trying to break patterns of thought that contribute to negative psychological states (Spain et al., 2020). Spain et al. (2020) state that CBT can be particularly helpful for autistic people, especially those with anxiety or obsessive-compulsive disorder (OCD) due to the formulaic structure of CBT, structured discussions that focus on practical details, collaboratively defined goals, and focus on implementing pragmatic strategies. Modified CBT has been one of the most helpful treatment options for up to 36% of autistic adults with substance use disorder, which is more common among social autistics without intellectual disability (Helverschou et al., 2019). For CBT to be effective for autistic people, there are accommodations that can be used to optimal use. To be most effective with literal minded autistic clients, practitioners can change session length to include enough time to discuss issues thoroughly and concretely, include more preparation and practical skill building, use repetition of tasks to create more comfortable routines that include special interests, and including other people in the client’s life such as family or teachers (Spain et al., 2020). These simple changes allow more comfort and practicality for autistic clients to implement CBT in their lives. Clinicians should also note that autistic clients may be more demanding and benefit from increased structure, more directive strategy implementation, high individualization of treatment, practical life support in areas of housing, life skills, and employment, and increased length and number of sessions compared to neurotypical clients (Helverschou et al., 2019). Exercise Simple remedies such as exercise can be helpful for autistic people and is associated in the general population with not only improved physical health but higher self-esteem, attention, self-efficacy, and reduced behavioral and emotional regulation problems (Tse, 2020). The ability to engage in physical tasks such as walking and exercise are associated with aging well and less health complications in autistic adults (Hwang et al., 2021). Tse (2020) states that for children with autism, exercise improved mood, emotional expression, emotional regulation, social functioning, and self-awareness, and decreased internal, and external behavioral problems such as stereotyped behaviors. These benefits may be due to serotonin, norepinephrine, and dopamine released by exercise that are associated with inhibition of behavior (Tse, 2020). While exercise is recommended as a healthy habit for all people, this can be especially important for mind-body integration and moderation of emotion in autism. Medication Treatments Due to differences in neurocognitive function among people with autism, medications often work differently for autistic people as compared to neurotypical people. Deb et al. (2021) state there is no evidence that older generation tricyclic antidepressant medications improve negative symptoms for autistic people and the risks of side effects and overdose make tricyclic antidepressants a poor choice for autistic people. They continue to state that research is lacking on anti-anxiety medications and newer antidepressants in the SSRI and serotonin-noradrenaline reuptake inhibitors group and only citalopram and buspirone have shown marginal benefit for autistic people, benzodiazepines and beta-blockers both have serious side effects and are not recommended for long term use. Overall, no significant benefits are seen for autistic people taking anti-depressants or anti-anxiety medications compared to placebo groups, which makes treatment for autistic adults difficult for modern medicine (Deb et al., 2021). Having no default medication recommendations for autistic people can be challenging to the modern medical system and requires more thoughtful consideration in treatment plans. Alternative Treatments With mainstream prescriptions found ineffective for treating autistic people with anxiety or depression or behavior and communication challenges, alternative treatments have been explored and found to be beneficial. Markopoulos et al. (2022) found that psychedelics such as lysergic acid diethylamide (LSD), psilocybin, and dimethyltryptamine (DMT), along with methylenedioxymethamphetamine (MDMA) have demonstrated ability to reduce social anxiety, increase pro-social behaviors, and increase empathy in autistic adults. For example, psylocibin has been found to increase openness and extraversion in people with treatment resistant depression up to three months after two sessions of therapy treatment. They continue to state LSD has been found to increase desire to be with other people, emotional empathy, sociability, trust, closeness, and blood levels of oxytocin. From the same study, LSD and psylocibin both reduce anxiety and depression symptoms and two therapy sessions of LSD allowed positive effects to last up to one year. Current research cannot say definitively if the use of psychedelics could be uniformly beneficial for autistic people due to the variety of symptomology and challenges autistic people experience and the possibility that the dysregulating effects of psychedelics would outweigh the prosocial benefits (Markopoulos et al., 2022). Cannabis has also shown positive outcomes to support autistic adults in escaping rigid maladaptive patterns of thought. Cannabis is associated with decreased hostile feelings and increased interpersonal communication ability (Aran et al., 2021). Aran et al. (2021) states that while THC can be associated with increased anxiety and psychosis and decreased motivation and cognitive decline, CBD seems to have antipsychotic, antiepileptic, and neuroprotective factors. They continue to say that cannabinoid treatment seems to improve social function and improve core challenges for 49% of autistic people compared to 21% who took a placebo. More research in alternative treatments would be beneficial as there are promising treatment options here. Applied Behavioral Analysis Applied behavioral analysis (ABA) is one of the more controversial treatments for autism. ABA consisting of analyzing behavior for antecedent, behaviors, and consequences, and using rewards and punishments to shape behaviors, and for many people in the United States it is the only treatment that insurance will pay for (Kirkham, 2017). While it has been found in research to be an effective treatment for some of the more challenging behaviors in autistic children, it is important to ask what criteria is being used to qualify studies as successful, children acting more typical or children learning strategies to live more full and happy lives (Tse, 2020). ABA has also been found to have caused complex PTSD in individuals who received classical ABA that utilize discrete trials, physical aversives, and repetition to replicate typical behavior from children at the cost of their own authentic behaviors, personality, judgment, and comfort (Kirkham, 2017). ABA done well with individualized therapies developed for each person has been shown to support autistic people in learning adaptive behaviors and coping strategies to deal with living in a world not designed for them, but treatment quality varies widely and there are ABA providers focused on contracts and monetary gain over the true benefit for the individual and their family, producing treatments that are less science-based, more harmful, and offer subpar benefits (Keenan et al., 2010). Kirkham (2017) points out that the modern neurodiversity movement claims ABA attempts to make autistic children act neurotypical, without concern for the mental health damage that repressing someone’s identity can have on a person. The same advocates claim autistic children do not require treatment just for being different from neurotypical people and ABA therapies should be carefully assessed before implementing on small children who are unable to defend themselves. Some posit that ABA done poorly trains children to be docile and do whatever adults demand, leading to autistic adults experiencing increased unwanted sexual experiences and sexual trauma as compared to neurotypical adults (Pecora et al., 2020). Research on adult autistic sexual experiences and ABA services received in childhood could answer this question more definitively. Evidence Based Treatment for Queer and Transgender Adults Transgender autistic people will often benefit from adapted treatment as communication and sensory challenges associated with autism and gender issues due to being transgender open the individual to discrimination and relational challenges on many fronts. According to Holt et al. (2021), 77% of transgender people seek therapy for gender identity issues and others seek therapy to manage internalized stigma, depression, anxiety, trauma, suicidal ideation, and substance use. It is often difficult for transgender people to find effective care as even providers from diverse sexually backgrounds may not understand diverse gender identities, and finding providers who accept and affirm the whole client and do not require the client to educate the provider on their gender identity is important (Snow et al., 2022). An important support for transgender youth is having parents and family that affirm and support their gender identity and provide them with access to gender-affirming treatment and family inclusion should not be neglected in treatment (Allen et al., 2021). Unfortunately, many of those who seek therapy will confront stigmatization from providers including misgendering and misunderstanding about gender in general that could be remedied by culturally responsive training for providers on transgender experiences and best practices in adapting treatment to meet transgender needs (Holt et al., 2021). Protective factors associated with transgender mental health are acceptance of self, self-esteem, being or having a role model, community and individual resources, and positive self-identity (Clements et al., 2021). Much like the autistic community, the transgender community also builds resiliency through technology such as social media posts, access to narratives and groups of other transgender people online, and intentional creation of a positive transgender self in a welcoming online environment before coming out in the brick and mortar world (Clements et al., 2021). Autistic LGBTQ+ people experience the double marginalization of being both autistic and queer and, as seen from previous research, autistic people are more likely to be bisexual. Wang and Feinstein (2022) found that bisexual individuals experience more mental health challenges, suicide risk, and substance abuse than either gay and lesbian and straight people but found protective factors that are worth exploring. They found that similarly to autistic resilience factors, support and acceptance from parents and peers, a sense of belonging, experiences with similar people, and positive self-identity development can reduce distress and internalized stigma and increase self-esteem and mental health. Embracing of bisexual identity is associated with increased mental health, resilience, positive associations with having unique perspectives, and ability to love without concern for sex or gender (Wang, & Feinstein 2022). Discussion for Section The neurodiversity movement is still relatively young and the idea that autistic people are simply different and not something to be corrected has not existed long enough for many solid research-based interventions to be evaluated on this premise. Evidence based treatments that have been found helpful for adult autistic queer people are practical lifestyle implementations of self-care, CBT, exercise, alternative treatments such as micro-dosing THC, LSD, or psylocibin, and therapy. Treatments that are controversial such as ABA should be given special attention before being implemented in a treatment plan. Although there is a wealth of research around families of autistic people and resilience, there is a lack of research on increasing resilience for autistic people themselves (Ghanouni & Quirke 2023) and what medications may reduce anxiety and depression for autistic people (Deb et al., 2021). More research needs to be done asking autistic people what they want to gain from treatment and what aspects of treatments they find most beneficial, much research is done in quantitative fashion and more qualitative information would be helpful in catering EBPs to autistic needs (Spain et al., 2020). Sample sizes for specialized research studies on autistic transgender individuals tend to be small and data collected is less reliable than larger sample sized would allow (Helverschou et al., 2019). Similarly, in research on alternative treatments using psychedelics, sample sizes from studies have been small, larger studies would need to be completed to know if possible side effect risks overwide the benefits from such treatments (Markopoulos et al., 2022). There may need to be different research into EBPs for people with and without intellectual disability and autism as effective treatments for these two autistic populations are likely to be different (Tse, 2020). While there is increasing research centered on transgender people, there are very few that look at non-binary populations by themselves and most transgender studies do not take into account sexuality among transgender people and how that may impact health (Holt et al., 2021).  REFERENCES Allen, L. R., Dodd, C. G., & Moser, C. N. (2021). Gender-affirming psychological assessment with youth and families: A mixed-methods examination. Practice Innovations, 6(3), 159–170. https://doi.org/10.1037/pri0000148 Aran, A., Harel, M., Cassuto, H., Polyansky, L., Schnapp, A., Wattad, N., Shmueli, D., Golan, D., & Castellanos, F. X. (2021). Cannabinoid treatment for autism: a proof-of-concept randomized trial. Molecular autism, 12(1), 6. https://doi.org/10.1186/s13229-021-00420-2 Bemmer, E. R., Boulton, K. A., Thomas, E. E., Larke, B., Lah, S., Hickie, I. B., & Guastella, A. J. (2021). Modified CBT for social anxiety and social functioning in young adults with autism spectrum disorder. Molecular Autism, 12, 1-15. doi:http://dx.doi.org/10.1186/s13229-021-00418-w Clements, Z. A., Rostosky, S. S., McCurry, S., & Riggle, E. D. B. (2021). Piloting a brief intervention to increase positive identity and well-being in transgender and nonbinary individuals. Professional Psychology: Research and Practice, 52(4), 328–332. https://doi.org/10.1037/pro0000390 Deb, S., Roy, M., Lee, R., Majid, M., Limbu, B., Santambrogio, J., Roy, A., & Bertelli, M. O. (2021). Randomised controlled trials of antidepressant and anti-anxiety medications for people with autism spectrum disorder: systematic review and meta-analysis. BJPsych open, 7(6), e179. https://doi.org/10.1192/bjo.2021.1003 Djela, M. (2021), Change of autism narrative is required to improve employment of autistic people, Advances in Autism, 7(1), 86-100. https://doi.org/10.1108/AIA-11-2019-0041 Doherty, M., Neilson, S., O'Sullivan, J., Carravallah, L., Johnson, M., Cullen, W., & Shaw, S. C. K. (2022). Barriers to healthcare and self-reported adverse outcomes for autistic adults: A cross-sectional study. BMJ Open, 12(2) doi:https://doi-org.csu.idm.oclc.org/10.1136/bmjopen-2021-056904 Ghanouni, P., & Quirke, S. (2023). Resilience and Coping Strategies in Adults with Autism Spectrum Disorder. Journal of autism and developmental disorders, 53(1), 456–467. https://doi.org/10.1007/s10803-022-05436-y Hall, J. P., Katie, B., Streed, C. G., Jr, Boyd, B. A., & Kurth, N. K. (2020). Health disparities among sexual and gender minorities with autism spectrum disorder. Journal of Autism and Developmental Disorders, 50(8), 3071-3077. https://doi-org.csu.idm.oclc.org/10.1007/s10803-020-04399-2 Helverschou, S. B., Brunvold, A. R., & Arnevik, E. A. (2019). Treating Patients With Co-occurring Autism Spectrum Disorder and Substance Use Disorder: A Clinical Explorative Study. Substance abuse : research and treatment, 13, 1178221819843291. https://doi.org/10.1177/1178221819843291 Holt, N. R., Ralston, A. L., Hope, D. A., Mocarski, R., & Woodruff, N. (2021). A systematic review of recommendations for behavioral health services for transgender and gender diverse adults: The three-legged stool of evidence-based practice is unbalanced. Clinical Psychology: Science and Practice, 28(2), 186–201. https://doi-org.csu.idm.oclc.org/10.1037/cps0000006.supp (Supplemental) Hwang, Y. I., Foley, K.-R., & Trollor, J. N. (2020). Aging well on the Autism spectrum: An examination of the dominant model of successful aging. Journal of Autism & Developmental Disorders, 50(7), 2326–2335. https://doi-org.proxy1.calsouthern.edu/10.1007/s10803-018-3596-8 Keenan, M., Dillenburger, K., Moderato, P., & Röttgers, H.-R. (2010). Science for sale in a free market economy: But at what price? Aba and the treatment of autism in europe. Behavior & Social Issues, 19(1), Pages 126–143. Kirkham, P. (2017). ‘The line between intervention and abuse’ – autism and applied behaviour analysis. History of the Human Sciences, 30(2), 107–126. https://doi.org/10.1177/0952695117702571 Markopoulos, A., Inserra, A., De Gregorio, D., & Gobbi, G. (2022). Evaluating the Potential Use of Serotonergic Psychedelics in Autism Spectrum Disorder. Frontiers in pharmacology, 12, 749068. https://doi.org/10.3389/fphar.2021.749068 Mayor A. (2021). Exploring the views of young people with autism spectrum disorder (ASD) on how to improve medical consultations. BJPsych Open, 7(Suppl 1), S207. https://doi.org/10.1192/bjo.2021.553 Pecora, L. A., Hancock, G. I., Hooley, M., Demmer, D. H., Attwood, T., Mesibov, G. B., & Stokes, M. A. (2020). Gender identity, sexual orientation and adverse sexual experiences in autistic females. Molecular Autism, 11, 1-16. https://doi-org.csu.idm.oclc.org/10.1186/s13229-020-00363-0 Snow, A., Cerel, J., & Frey, L. (2022). A safe bet? Transgender and gender diverse experiences with inclusive therapists. The American journal of orthopsychiatry, 92(2), 154–158. https://doi.org/10.1037/ort0000599 Spain, D., Happé, F. How to Optimise Cognitive Behaviour Therapy (CBT) for People with Autism Spectrum Disorders (ASD): A Delphi Study. J Rat-Emo Cognitive-Behav Ther 38, 184–208 (2020). https://doi.org/10.1007/s10942-019-00335-1 Tse A. C. Y. (2020). Brief Report: Impact of a Physical Exercise Intervention on Emotion Regulation and Behavioral Functioning in Children with Autism Spectrum Disorder. Journal of autism and developmental disorders, 50(11), 4191–4198. https://doi.org/10.1007/s10803-020-04418-2 Wang, A. Y., & Feinstein, B. A. (2022). The perks of being bi+: Positive sexual orientation-related experiences among bisexual, pansexual, and queer male youth. Psychology of sexual orientation and gender diversity, 9(1), 58–70. https://doi.org/10.1037/sgd0000459 Disproportionate Health Impacts For Queer Autistic Adultsby Lisa Macafee Disproportionate Mental Health Impacts of Being Transgender And Autistic LGBTQ+ autistic people experience disproportionate impacts of being double marginalized. Many adults are getting autism diagnosis later in life due to increasing awareness of different types of autism presentation and changes in the DSM-V that allow for a broader understanding and diagnosis of autism (Stagg & Belcher, 2019). Autistic adults compared to neurotypical adults have higher rates of substance abuse disorder, diagnosis of depression, ADHD, anxiety (especially social anxiety), and obsessive compulsive disorder (OCD), in addition to increased rates of chronic health conditions (Colvert et al., 2022). LGBTQ+ individuals, and especially transgender people, have higher rates of mental health challenges, especially anxiety, depression, and PTSD (Hall et al., 2020). Autism and Mental Health Autistic people are 15 times more likely when compared to the general public to have a mental health concern, and more autistic traits scale with more mental health concerns (Colvert et al., 2022). 20% of autistics have anxiety diagnosis, 16.1% psychotic disorders, 14.9% personality disorders not otherwise specified, 13.7% have depression, 9% have OCD, 5% bipolar disorder and 4% have schizophrenia spectrum disorders, and an unknown number of autistic people are misdiagnosed with things like ADHD when an autism diagnosis would allow for more appropriate supports (Fusar-Poli et al., 2022). 3.2% of severe psychiatric inpatients have autism and it is estimated that between 2.4% and 9.9% of patients in psychiatric hospitals would qualify for an autism diagnosis, and without it, are being treated for misidentified problems and in ways that may not be as supportive as autism accommodations could be, and AMAB are more likely to get ADHD, psychosis, or conduct disorders, while AFAB are more likely to get depression, anxiety, and personality disorder diagnosis (Fusar-Poli et al., 2022). 31%-70% of autistic youth have at least one additional mental health diagnosis and 27%-41% have two or more diagnosis in addition to autism (Colvert et al., 2022). Between 27% and 42% of autistic adults experience anxiety in their lifetime, 23% to 37% depression, 11% to 66% experience suicidal ideation and between 1% and 35% attempt suicide (Fusar-Poli et al., 2022). Autistic people are at particular risk of early death and die an average of 16 years earlier than average, with the largest cause of early death being suicide (Moseley et al., 2021). Autistic people are 7.55 times more likely to commit suicide and autistic adults without intellectual disability are nine time more likely to commit suicide (Fusar-Poli et al., 2022). Autistic adults generally experience more physical, social, and psychological stressors than neurotypical adults and feel the impact of these stressors more intensely, which correlates to increased risks of mental health challenges (Moseley et al., 2021). Autistic people experience sensory processing differences that vary in intensity and type by individual that often make cognitive, motor, and social skills tasks more challenging when also navigating a sensory issue such as tactile sensitivity, like tags in shirts, taste and smell sensitivity, such as aversion to someone wearing perfume, movement sensitivity, such as being on a high floor of a building or on a bus, auditory filtering, such as hearing the rattle of an air conditioning vent above all other input, hyposensitivity and sensation seeking behaviors, visual and auditory sensitivity, such as things being too bright or too loud, low energy, and weakness (Scheerer et al., 2021). Chronic stress impairs executive function, self-regulation, and coping skills, which all can lead to more stressors, creating a cyclical problem (Moseley et al., 2021). Autistic people are at particular risk of this kind of stress cycle because they often know they are missing cues, but are not sure which cues have been missed, leading to hyper-vigilance and increased response to stressors, such as worrying about what was said and if a corrective response is needed or would make things worse. Loneliness, chronic anxiety, and lack of social supports increase the physical and mental health impacts of stressors, but for many autistic people, navigating loneliness is common due to social communication challenges and inability to maintain meaningful social relationships that cause autistic adults to be socially isolated (Moseley et al., 2021). Loneliness in autism is related to higher perception of stress, suicide, self-harm, and mental health challenges and may be due to less ability to moderate stressors through social relationships and higher likelihood to use maladaptive coping strategies without social support (Moseley et al., 2021). Autistic children are more likely to live in poverty, experience child sexual abuse, parent illness, substance abuse, and divorce, which all negatively impact mental health (Moseley et al., 2021). Autistic people experience high rates of childhood bullying which can affect development of healthy social lives, relationship difficulties, and victimization (Moseley et al., 2021). Autistic adults are also more likely to be socially stigmatized, be underemployed or unemployed, have contact with the criminal justice system, and be victims of physical, sexual, or emotional exploitation due to naivete (Moseley et al., 2021). 62% of autistic adults state that they are unable to secure appropriate supports for themselves (Stagg & Belcher, 2019). Things that would not seem as stressful to the average person, such as changes in routine or plans can be highly stressful for an autistic person and cause days of rumination on the unpredictability of a situation experienced, a physically dangerous experience like a near car crash, or humiliating social situations long past (Moseley et al., 2021). Autistic people’s perception of the intensity of interpersonal loss, entrapment, and role change or disruption negatively impact mental health, and these perceptions can be impacted by rigid thinking, lack of emotional awareness, poor coping skills, and self-advocacy skills (Moseley et al., 2021). These being noted, it does appear that ritualistic behavior and routines associated with OCD diagnosis do lessen in intensity as autistic individuals grow into adulthood (Scheerer et al., 2021). Autism diagnoses in adults are made an average of 11 years after an individual first sought mental health support, 66.5% of autistic adults received other diagnosis before autism that were often symptomatic of untreated autism, such as anxiety, depression, psychoses, and personality disorders (Fusar-Poli et al., 2022). Many late-diagnosed adults, often called the lost generation, were previously diagnosed with anxiety and depression and had feelings of isolation and alienation that allowed for an autism diagnosis to be perceived as a positive, allowing for identification of factors that individuals now can accommodate for (Fusar-Poli et al., 2022; Stagg & Belcher, 2019). Individuals receiving a diagnosis later in life often are confronted with relief, but also a need to re-shape self-concept as autistic and change the ways that they have thought about themselves to make sense of life experiences including loneliness, difficulty making friends and maintaining relationships, feeling different from others, and ways to cope with stressors previously misunderstood outside the autism context (Stagg & Belcher, 2019). While some late-diagnosed autistics viewed it as a positive, there is no unified autistic response, some people found the diagnosis disturbing and felt it impacted their self-esteem in negative ways, while others felt it was revelatory to gain new insights into their previously alien-seeming behaviors and emotional regulation challenges (Stagg & Belcher, 2019). Autistic AFAB are diagnosed four years later in life on average than ABAB due less informed diagnostic practices for women and higher camouflaging skills that hide autistic traits at the expense of getting appropriate care, which is associated with worse health outcomes (Fusar-Poli et al., 2022; Moseley et al., 2021). Autistic AFAB people are often better at camouflaging or masking to meet the demands of the neurotypical world than autistic men, but masking is associated with higher stress levels, exhaustion, and increased anxiety when compared to autistics who do not camouflage (Milner et al., 2019). AFAB autistics are more likely to internalize their autistic traits, which can appear more similar to anxiety and depression, causing misdiagnosis, missed diagnosis, and inappropriate supports offered (Fusar-Poli et al., 2022). Queer and Transgender Mental Health Transgender people experience direct impacts to mental health, such as discrimination and hate crimes, and indirect impacts, including social exclusion, microaggressions, microinsults, and microinvalidations, with twice the rate of mental health diagnosis as compared to cisgender peers (Pinna et al., 2022; Wesselmann et al., 2022). Transgender people have 1.5 times the number of mood disorders, 3.9 times the number of anxiety disorders, and 3.8 times the rate of psychotic disorders (Pinna et al., 2022) and experience heightened levels of discrimination with 63% experiencing one or more serious act of discrimination and 23% experiencing three or more acts of serious discrimination (Gleisberg et al., 2022). Living through such stressors may prompt hyper-vigilance to be able to avoid stressors, hiding of gender identity, and internalization of negative views expressed towards them by society which can lead to mood disorders, substance use, and suicidal ideation (Pinna et al., 2022). Social exclusion, including interpersonal rejection, being told their presence is undesired, or being laughed at, has negative physical and mental health impacts similar to the impact that loneliness has on autistic people (Wesselmann et al., 2022). Transgender people also face discrimination in employment and housing and are more likely to be unemployed, possibly leading to higher rates of sex work, particularly for transgender women, and substance use in the transgender population, with 75% using alcohol and one third using multiple substances (Pinna et al., 2022). Chronic exclusion can lead to increased anger, sadness, devaluation of self, feelings of inhumanity, depression, alienation, suicidal ideation, and self-harm (Wesselmann et al., 2022). One fourth of transgender youth experience clinical levels of anxiety and depression, one third experience family dysfunction, and one-eighth of transgender youth attempts suicide, thirteen times more often than cisgender peers (Pinna et al., 2022). Queer and transgender people are often navigating their intersectional identities of race, gender, sexuality, and disability and often need to decide which identities to express and which may not be safe or welcomed identities to express, at any given time ,of their multiple marginalized identities (Garvey et al., 2019). While previous studies have demonstrated the stressors that transgender women experience due to safety concerns, transgender men often experience heightened social anxieties due to fear of not being seen as masculine or not having learned the male social role well enough (Nobili et al., 2018). While mental health care providers are often open to providing gender-inclusive care, fewer than a third of psychologists say they have received appropriate training or experience needed to do so, leading to a high unmet need in care (Pinna et al., 2022). Controversy exists for some families of transgender youth in thinking their transgender identity is a phase, some families do not allowing gender affirming care, medical, or social transitioning, and many gender creative youth are shamed for their behaviors, which have negative mental health impacts (Ashley, 2022). Social transitioning, even without medical transitioning of any kind, reduces anxiety and depression to rates comparable to cisgender peers, medical transition is not necessary to reduce mental health disparities (Ashley, 2022). Transgender adults are not uniform in manner or desire for transition, 22% are undecided on or do not want hormone replacement therapy, and about one third of transgender individuals identify as non-binary and may have no desire for medical transition at all (Ashley, 2022). That being said, between 96.5% and 100% of youth who used hormone blockers to prevent their assigned sex hormones from causing puberty perused gender replacement hormone therapy later and 96% of youth continue to refer to themselves as transgender into late adolescence (Ashley, 2022). Another identity more common amongst autistic adults is asexuality, or having little to no drive for sexual relations, which became more common and better understood with the proliferation of social media and online communities (Mollet, 2023). People identifying as asexual often feel unwelcome in LGBTQ+ communities, who are often celebrating their sexual attraction to same sex, multiple genders, or transgender identities and can feel lack of belonging and invalidation (Mollet, 2023). Asexuality has been met with dehumanizing views from peers that are not directed at lesbian or gay identities anymore, and asexual people are often avoided by straight and gay peers alike (Mollet, 2023). Some asexual people fear disclosing their identity because they do not know how it will be perceived, some people have been cut off from friends and family when disclosing asexual identity, leading to negative well-being and interpersonal relationship challenges (Mollet, 2023). Disproportionate Physical Health Impacts of Being Queer or Transgender And Autistic Autism And Physical Health Impacts Autistic adults die an average of 16-38.5 years earlier than neurotypical adults and autistic adults, especially autistic AFAB adults, have trouble with eating a healthy diet, weight (both over and underweight), exercise, sleep troubles, have elevated rates of diabetes, cancer, respiratory conditions, and heart disease (Doherty et al., 2022; Weir et al., 2021). Eating well can be a challenge for autistic adults as up to 70% of autistic children have food challenges due to sensitivities, allergies, and inflexibilities, including avoidant restrictive food intake disorder (ARFID), anorexia, pica, and food refusal, and changing habits in adulthood is not always easy to do (Weir et al., 2021). Exercise and sleep are areas of concern, autistic children engage less in outdoor activities than neurotypical peers, autistic AFAB exercise even less as they get older, and autistic people are more likely to have sleep disorders, the severity of which scale with challenging autistic traits (Weir et al., 2021). Sleep challenges in autistic adults are associated with unemployment, increased mental health challenges, and sedentary behavior, which may increase physical health challenges and obstruct social engagements, making healthy sleep habits and management of autistic traits more difficult to attain (Weir et al., 2021). Autistic adults, especially AFAB, are more likely to have chronic health troubles including chronic fatigue syndrome (CFS), fibromyalgia, chronic migraines, irritable bowel syndrome (IBS), restless leg syndrome (RLS), and temporomandibular joint disorder (TMJD), collectively referred to as central sensitivity syndrome (CSS) disorders, as all of these disorders include chronic pain, fatigue, and hyper-sensitization (Grant et al., 2022). 60% of autistic adults demonstrate clinical signs of having CSS, compared to up to 20% of the general population, and the CSS collection of health challenges scale with increased sensory sensitivity, greater anxiety, and less well-being (Grant et al., 2022). Autistic adults and people who experience CSS are associated with mental health challenges, trauma, discrimination, and lack of access to or poor experiences with healthcare (Grant et al., 2022). Autistic adults are more likely to have joint hypermobility disorders that often co-occur with CSS and higher rates of sensory sensitivity and anxiety associated with autism increase rates of CSS (Grant et al., 2022). Anxiety, stress, and PTSD, all more common to autistic people, may not only increase rates of CSS, but severity of the symptoms, and may be made worse by less developed coping mechanisms in autistic people (Grant et al., 2022). Autistic AFAB are more likely than autistic AMAB or neurotypical women to experience higher sensory sensitivities (Grant et al., 2022). Autistic adults are also more likely to have dysautonomia and mast cell activation syndrome (Grant et al., 2022). Chronic stress can suppress the immune system, impact brain plasticity, epigenetic expression of genes, increase cardiovascular, autoimmune, and neurodegenerative concerns, and can cause over sensitization of the stress response (Moseley et al., 2021). Long-term activation of the stress response can cause many health concerns and autistic adults are more likely to experience epilepsy, diabetes, gastrointestinal concerns, hypertension and immune system complications (Moseley et al., 2021). Causes of adverse health outcomes are partly caused by challenges with social-emotional responses such as maintaining relationships, but can also be attributed to long-term medication use, health care access barriers, as well as genetic causes (Moseley et al., 2021). The perceived severity of physically dangerous stressors such as an armed robbery at a convenience store negatively impacts the physical health of autistic people (Moseley et al., 2021). Accessing appropriate healthcare is more difficult for autistic adults, which may be part of the reason autistic adults experience adverse health outcomes as compared to neurotypical adults (Doherty et al., 2022). 80% of autistic adults reported difficulty going to a general practitioner, 72% have difficulty deciding if they should go to the doctor, 62% have difficulty making appointments on the phone, 56% feel they are misunderstood, 53% have difficulty communicating with their doctor, and 51% have challenges with the waiting room (Doherty et al., 2022). Doherty et al. (2022) also found that autistic people are twice as likely to use emergency room services, are more likely to die in the ER, and are three times as likely to need inpatient care due to not getting early preventative care, not attending specialist referral appointments, and untreated life-threatening conditions. They also found that these numbers may be exacerbated because only 20% of healthcare providers said that they had confidence in being able to communicate with and identify and implement appropriate accommodation for autistic adults. Communication problems with medical providers are complicated by anxiety and sensory issues associated with autism and some autistic people do not self-disclose autism to their doctors, preventing access to appropriate accommodations and care (Doherty et al., 2022). Queer and Transgender Physical Health Impacts LGBTQ+ people have higher rates of health challenges and face barriers to accessing appropriate care due to their marginalized identities (Hall et al., 2020). 60% of trans and non-binary adults reported having a long-term health condition, with autism, dementia, learning disability, and metal health being the most disproportionately reported, and stroke, diabetes, and kidney or liver problems increasing with age at disproportionate rates compares to straight cisgender individuals (Saunders et al., 2023). LGBTQ+ people are less likely to have a regular medical provider that they see and are more likely to be homeless, which is associated with negative health impacts (Saunders et al., 2022). Trans and non-binary adults report having poor experiences in healthcare than straight cisgender adults, but these results are mitigated when they receive treatment from healthcare providers knowledgeable about transgender health (Saunders et al., 2023). Health disparities, especially mental health disparities between transgender and cisgender people decrease with age, possibly suggesting that as they age, transgender people develop coping skills, find better access to health care, or feel better the longer they are on gender affirming therapies (Saunders et al., 2023). Exposure to chronic environmental stressors and discrimination has negative health impacts on transgender people (Pinna et al., 2022). 10% of transgender people experience sexual assault due to their transgender identity, 80% reported verbal abuse, 60% sexual abuse, and more than 30% reported physical abuse of some kind (Pinna et al., 2022). Transgender adults as compared to cisgender adults have higher rates of trauma, PTSD, anxiety, depression, and physical health concerns. Transgender women have a higher mortality rate due to suicide, heart disease, lung cancer, and HIV (Pinna et al., 2022). Discussion for Section Physical and mental health are impacted for individuals who are both autistic and LGBTQ+ and there is a disproportionate impact on trans autistic health. Queer autistic people face a double-marginalization and navigate discrimination from being LGBTQ+ and from being autistic, leading to worse mental and physical health than either straight cis-gender autistic people or LGBTQ+ neurotypical people (Hall et al., 2020). Autistic LGBTQ+ adults face exponential challenges due to the social communication challenges associated with autism directly impacting the individual’s ability to secure gender affirming care, advocate for themselves in mental health care, and navigate personal and professional relationships. Transgender autistic AFAB often experience increased social challenges associated with mental flexibility, social skills, and switching attention, which often leads to heightened social anxiety health impacts (Nobili et al., 2018). LGBTQ+ autistics are twice as likely to have a mental health concern, have more than double the days of poor physical health, smoke ten times as much, have higher unmet healthcare needs, and 37% have been refused care from a healthcare provider compared to 20% of straight cisgender autistics (Hall et al., 2020). Autistic transgender people experience minority stressors due to challenges from these intersecting identities, including challenges securing gender affirming health care due to their autism diagnosis (Cooper et al., 2022). Autistic transgender adults experience more discrimination than transgender neurotypical or autistic cisgender individuals (Cooper et al., 2022). Much of the research used looks at either LGBTQ+ or autistic adults and few studies have been done looking at the cross-section of individuals who are both. Much of the research looking at trans autistic people is done in youth hospitals, which may skew the results. More research is needed on the experiences of transgender AFAB and mental health impacts from stressors. Research is needed to determine if a large percentage of transgender people are autistic or if trauma that transgender people often experience mimics autistic traits as social anxiety and difficulty switching attention can be caused from trauma and autism (Nobili et al., 2018). Some studies on autistic adults screen for adults with autism but without intellectual disability and some studies include both groups in studies, it is unclear if autistic adults without intellectual disability may yield very different research results than autistic adults with intellectual disability, but is there are large differences, it would be good to have results with the screen in place (Weir et al., 2021). While there has been adequate research on autistic or LGBTQ+ disproportionate impacts, there is not a wealth of research focusing on autistic LGBTQ+ individuals. Many of the studies focusing on autism and mental health are done with clinical samples of more intense support-need individuals and of children or autistic youth with autistic adults not as well covered (Colvert et al., 2022). Another issue is survey results are often completed by parents or caregivers of autistic people and not by the autistic person themselves, which may result in inaccurate information being presented (Scheerer et al., 2021). Although there are a number of transgender and non-binary researchers, the majority of research on transgender issues is done by cisgender people, which may bring about misunderstandings or inaccurate concepts of gender identity, such as confusing sex, sexuality, and gender (Gleisberg et al., 2022). There is a need for research questions to be phrased in neutral terms as some people from marginalized identities will not respond to survey questions that are further stigmatizing, for example, if answering a question that is phrased in a stigmatizing way, people who may identify with what is being asked may decline to respond because they don’t like the way the question makes them feel, which prevents accurate data collection (Saunders et al., 2022), this is particularly true for autistic individuals who may be more sensitive to their inability to control their image and perception by society than neurotypical people.  REFERENCES
Ashley, F. (2022). The clinical irrelevance of “desistance” research for transgender and gender creative youth. Psychology of Sexual Orientation and Gender Diversity, 9(4), 387–397. https://doi.org/10.1037/sgd0000504 Cooper, K., Mandy, W., Butler, C., & Russell, A. (2022). The lived experience of gender dysphoria in autistic adults: An interpretative phenomenological analysis. Autism, 26(4), 963-974. https://doi-org.csu.idm.oclc.org/10.1177/13623613211039113 Colvert, E., Simonoff, E., Capp, S. J., Ronald, A., Bolton, P., & Happé, F. (2022). Autism Spectrum Disorder and Mental Health Problems: Patterns of Difficulties and Longitudinal Trajectories in a Population-Based Twin Sample. Journal of autism and developmental disorders, 52(3), 1077–1091. https://doi.org/10.1007/s10803-021-05006-8 Doherty, M., Neilson, S., O'Sullivan, J., Carravallah, L., Johnson, M., Cullen, W., & Shaw, S. C. K. (2022). Barriers to healthcare and self-reported adverse outcomes for autistic adults: A cross-sectional study. BMJ Open, 12(2) doi:https://doi-org.csu.idm.oclc.org/10.1136/bmjopen-2021-056904 Fusar-Poli, L., Brondino, N., Politi, P., & Aguglia, E. (2022). Missed diagnoses and misdiagnoses of adults with autism spectrum disorder. European archives of psychiatry and clinical neuroscience, 272(2), 187–198. https://doi.org/10.1007/s00406-020-01189-w Garvey, J. C., Mobley, S. D., Summerville, K. S., & Moore, G. T. (2019). Queer and Trans* Students of Color: Navigating Identity Disclosure and College Contexts. Journal of Higher Education, 90(1), 150–178. https://doi-org.csu.idm.oclc.org/10.1080/00221546.2018.1449081 Gleisberg, A. I., Pacha, K., Chang, S., Erickson-Schroth, L., Johnson, K., & Luz Hernandez, S. (2022). Surveying trans and nonbinary communities: Research methodologies, accountability, and ethics with the Trans Bodies, Trans Selves Survey (2nd edition). Psychology of Sexual Orientation and Gender Diversity. Advance online publication. https://doi.org/10.1037/sgd0000575 Grant, S., Norton, S., Weiland, R. F., Scheeren, A. M., Begeer, S., & Hoekstra, R. A. (2022). Autism and chronic ill health: an observational study of symptoms and diagnoses of central sensitivity syndromes in autistic adults. Molecular autism, 13(1), 7. https://doi.org/10.1186/s13229-022-00486-6 Hall, J. P., Katie, B., Streed, C. G., Jr, Boyd, B. A., & Kurth, N. K. (2020). Health disparities among sexual and gender minorities with autism spectrum disorder. Journal of Autism and Developmental Disorders, 50(8), 3071-3077. https://doi-org.csu.idm.oclc.org/10.1007/s10803-020-04399-2 Milner, V., McIntosh, H., Colvert, E., & Happé, F. (2019). A Qualitative Exploration of the Female Experience of Autism Spectrum Disorder (ASD). Journal of autism and developmental disorders, 49(6), 2389–2402. https://doi.org/10.1007/s10803-019-03906-4 Mollet, A. L. (2023). “It’s easier just to say I’m queer”: Asexual college students’ strategic identity management. Journal of Diversity in Higher Education, 16(1), 13–25. https://doi.org/10.1037/dhe0000210 Moseley, R. L., Turner-Cobb, J. M., Spahr, C. M., Shields, G. S., & Slavich, G. M. (2021). Lifetime and perceived stress, social support, loneliness, and health in autistic adults. Health psychology : official journal of the Division of Health Psychology, American Psychological Association, 40(8), 556–568. https://doi.org/10.1037/hea0001108 Nobili, A., Glazebrook, C., Bouman, W. P., Glidden, D., Baron-Cohen, S., Allison, C., Smith, P., & Arcelus, J. (2018). Autistic Traits in Treatment-Seeking Transgender Adults. Journal of Autism & Developmental Disorders, 48(12), 3984–3994. https://doi-org.csu.idm.oclc.org/10.1007/s10803-018-3557-2 Pinna, F., Paribello, P., Somaini, G., Corona, A., Ventriglio, A., Corrias, C., Frau, I., Murgia, R., El Kacemi, S., Galeazzi, G. M., Mirandola, M., Amaddeo, F., Crapanzano, A., Converti, M., Piras, P., Suprani, F., Manchia, M., Fiorillo, A., Carpiniello, B., & Italian Working Group on LGBTQI Mental Health (2022). Mental health in transgender individuals: a systematic review. International review of psychiatry (Abingdon, England), 34(3-4), 292–359. https://doi.org/10.1080/09540261.2022.2093629 Saunders, C. L., Berner, A., Lund, J., Mason, A. M., Oakes-Monger, T., Roberts, M., Smith, J., & Duschinsky, R. (2023). Demographic characteristics, long-term health conditions and healthcare experiences of 6333 trans and non-binary adults in England: nationally representative evidence from the 2021 GP Patient Survey. BMJ Open, 13(2)https://doi-org.csu.idm.oclc.org/10.1136/bmjopen-2022-068099 Saunders, C. L., Lund, J., Mason, A. M., Roberts, M., Smith, J., & Duschinsky, R. (2022). The Health and Healthcare Outcomes of Trans and/or Non-Binary Adults in England: Protocol for an Analysis of Responses to the 2021 GP Patient Survey. Sexes, 3(3), 325–335. https://doi.org/10.3390/sexes3030025 Scheerer, N. E., Curcin, K., Stojanoski, B., Anagnostou, E., Nicolson, R., Kelley, E., Georgiades, S., Liu, X., & Stevenson, R. A. (2021). Exploring sensory phenotypes in autism spectrum disorder. Molecular autism, 12(1), 67. https://doi.org/10.1186/s13229-021-00471-5 Stagg, S. D., & Belcher, H. (2019). Living with autism without knowing: receiving a diagnosis in later life. Health psychology and behavioral medicine, 7(1), 348–361. https://doi.org/10.1080/21642850.2019.1684920 Weir, E., Allison, C., Ong, K. K., & Baron-Cohen, S. (2021). An investigation of the diet, exercise, sleep, BMI, and health outcomes of autistic adults. Molecular autism, 12(1), 31. https://doi.org/10.1186/s13229-021-00441-x Wesselmann, E. D., DeSouza, E. R., AuBuchon, S., Bebel, C., & Parris, L. (2022). Investigating microaggressions against transgender individuals as a form of social exclusion. Psychology of Sexual Orientation and Gender Diversity, 9(4), 454–465. https://doi.org/10.1037/sgd0000513 Sex, Gender, And Sexuality Diversity Among Autistic Adults by Lisa Macafee Autistic people have been shown through numerous studies to have higher rates of transgender, non-binary, gender diversity, and gender non-conforming identities and there are also heightened rates of autistic traits in the transgender community. Gender variance in autistic individuals assigned female at birth (AFAB) have the highest rates of gender, sex, and sexuality variance (Kung, 2020). Biological sex differences present among autistic adults assigned male at birth (AMAB) and AFAB are discussed, including sex trait atypicality and intersex traits more frequently present among AFAB autistics. Sexuality in autistic adults, including increased rates of asexuality, a-romanticism, pansexuality, demisexuality, bisexuality, gay, lesbian, same-sex-loving, and polyamorous identities is discussed. Autism and Gender Diversity Gender for autistic people is often perceived as a spectrum of many genders rather than a male/female binary and with an understanding that a person’s gender identity will develop differently due to the biological nature of the person, the culture they were raised in, how supported they are in their home, and will change over time and should not be considered static (Ehrensaft, 2018). Autistic people are six to eight times more likely to be transgender or gender non-conforming (Warrier, et. all, 2020) and transgender people are three to six times more likely to be autistic (Cooper, et. all, 2022). 11.3% of autistic adults express gender variance as compared to 0.7%-5% of the neurotypical population (Pecora, et. all, 2020). These differences are thought to be due to autistic resistance to social conditioning around gender and not feeling compelled to conform to gender norms as neurotypical individuals may feel the need to do (Cooper, et. all, 2022). Autistic individuals are 7.76 times more likely than neurotypical individuals to wish they were the opposite sex from what they were assigned at birth, with about 5% of autistic people wishing they were opposite gendered than they are (Janssen, et. all, 2016). Some of this gender flexibility may be due to rigid thinking associated with autism and a logical deduction that if gender expectations are not 100% met for the autistic person’s assigned sex at birth, then that logically may cause them to adopt a transgender or non-binary gender identity because they don’t fit with gender stereotypes (Pecora, et. all, 2020). Gender Diversity and AFAB Autistics Autistic people are more likely to be gender non-conforming or transgender and often experience gender stress and social anxiety due to their gender identity (Ehrensaft, 2018). Autistic people may not experience gender at all, they may express and experience gender differently as a neurodivergent individual and while understanding they are told they are a boy or a girl, may have very little affinity or alignment with gendered terms until puberty forces a physical reckoning with gendered roles and often a consequent rejection of expectations (Ehrensaft, 2018). AFAB autistic adults have the highest rates of gender flexibility and often present a masculinized autism profile, while AMAB autistics did not show a feminine autism profile (Kung, 2020). Gender roles can be confusing or irrelevant to autistic people, and some autistic AFAB people adopt masculine presentation because it is simpler, involves less social navigation, and is easier to navigate than wearing make-up and fashionable women’s clothing (Milner, et. all, 2019). Impaired social navigation associated with autism may have led to difficulties for AFAB autistics to socialize with women and increase the likelihood of socializing more with men and associating the self more with a male gender identity (Jones, et. all, 2012). Lastly, AFAB autistics often experience autism related challenges in socialization that make it difficult to maintain friendships with neurotypical girls, which often leads to friendships with men because they typically engage in less small talk, emotional discourse, are more socially forgiving than women, leading to a more male gendered experience (Milner, et. all, 2019). 15% of autistic adults report a transgender or non-binary gender identity with 21.6% of AFAB autistics reporting a transgender identity with only 4% of transgender AFAB autistic people identify on the male/female binary, 96% of AFAB transgender autistics identified as non-binary, which leads to speculation regarding why gender identity leans away from the binary in AFAB autistics (Walsh, et. all, 2018). The gender flexibility that autistic people often experience aligns with the fact that non-binary people have the highest rates of autism as compared to all other gender identity groups, the resistance to social conditioning that autistic people often experience may lend to their adopting unconventional gender identities that neurotypical people may not have felt comfortable acting as, even if they felt aligned to that gender identity (Walsh, et. all, 2018). It could be simply that autistic people are less prevented from expressing their inner transgender or non-binary identity due to less social constraints and conditioning than neurotypical people. Autistic AFAB people may express their gender identity in less typical ways due to the lack of inherent social expectation internalization, whether they are transgender (such as being more likely to be non-binary), or if they are cisgender, by being gender non-conforming and engaging in masculine behaviors or gender performance because it is more comfortable or less demanding than the female gender role performance expectations (Janssen, et. all, 2016). Autism and Transgender Identities Transgender people overall are about eight times more likely to be autistic than the cisgender population, and youth are more likely to identify outside the gender male/female binary and embrace a gender spectrum instead of a gender binary (Ehrensaft, 2018). Transgender adults overall are 3.03-6.36 times as likely to be autistic as compared to cisgender people and also reported they did not feel the need to conform to gender stereotypes for their gender identity (Cooper, et. all, 2022). Transgender AFAB men are 11 times more likely to qualify for an autism diagnosis than cisgender men (Jones, et. all, 2012). Transgender and non-binary AFAB adults are twice as likely to qualify for an autism diagnosis compared to cisgender women (Nobili, et. all, 2018). More than a third of transgender AFAB people meet autism diagnostic cut-off rates (Nobili, et. all, 2020), which is much higher than the less than one percent rates of transgender AMAB and cisgender people (Cooper, et. all, 2022; Heylens et al., 2018; Jones et al., 2012; Nobili et al., 2018). Transgender men scored 9.02 standard deviations higher and non-binary AFAB scored 8.38 standard deviations higher on the autism quotient survey than cisgender people (Kung, 2020). 15% of transgender men, 19% of non-binary AFAB, 3% of transgender women, and 2% of non-binary AMAB meeting the cut-off point for a likely autism diagnosis (Kung, 2020). Autism is diagnosed in 6% of transgender individuals, which is six times higher that the typical rate of autism and if criteria is expanded to look at a broader autism phenotype, 19.4% of gender diverse youth have elevated autistic traits (Heylens, et. all, 2018). Transgender and gender diverse individuals have high rates of autism, other neurodevelopmental disorders such as ADHD, and higher rates of psychiatric diagnosis such as anxiety, depression, obsessions compulsive disorder (Cooper, et. all, 2022; Warrier, et. all, 2020). Autism and Sexuality Autistic adults, especially those AFAB, show increased flexibility in sexuality, which can be thought of as a combination of sexual identity, sexual attraction, and sexual contact (Pecora, et. all, 2020). 15%-35% of autistic adults overall reported exclusively gay or bisexual orientations compared to 5.4% of neurotypical adults (Pecora, et. all, 2016). Some propose that the lack of internalized social rules autistic people experience allows them to engage in acts where neurotypical people prevent themselves from acting differently than they have been taught is socially acceptable. In a sense, not internalizing social norms may allow autistic people to be more flexible in their thoughts and actions than neurotypical adults. Autistic adults are associated with higher rates of gender and sexuality diversity, identities that have both increased in frequency, possibly due to increased ability to build online communities that normalize differences and allow discourse and healthy identity building for marginalized groups (Øien, et. all, 2018). Autism and Lesbian, Gay, Bisexual, and Pansexual Identities AFAB autistics identify as bisexual four times more frequently than neurotypical women and this is more frequently combined with masculine gender role expression and more of a male gender identity (Pecora, et. all, 2016). In addition, AFAB autistics are 2.39 times more likely to be gay or lesbian and 2.33 times more likely to be bisexual as compared to neurotypical women (Pecora, et. all, 2020). AFAB autistic people are more likely to be attracted to multiple genders and be gender non-conforming themselves (Dewinter, et. all, 2017). Gender flexibility in the self could influence sexuality in that if the individual themself does not abide by binary gender roles, it may be easier to disregard or expand upon which gender a person is attracted to. About half of AFAB autistic adults are in relationships, most living with their partner (Dewinter, et. all, 2017) but many autistic people experience challenges finding and maintaining sexual and romantic partnerships (Pecora, et. all, 2020). Many autistic people turn to the internet for sex education, which can further harm their understanding of appropriate behavior in relationships an encourage inappropriate behaviors (Maggio, et. all, 2022). This lack of sexual access and information could influence some autistic people to broaden their search for partners into genders that, if they were more socially able to find partners, they would not have considered, leading to sexuality flexibility, and in others can lead to inappropriate or dangerous sexual activity (Gilmour, et. all, 2012). Autistic traits seem to complicate sexual orientation and identification or make it easier to identify outside typical expectations (Maggio, et. all, 2022). Individuals who identify with bisexual (attracted to both men and women) or pansexual (attracted to all genders) identities often are aware of their sexuality later than gay or lesbian individuals, which could add to confusion or flexibility for autistic adults (Bishop et. all, 2020). Autism and Asexual, Aromantic, Polyamorous, and Other Queer Identities AFAB autistics have less sexual desire, less sexual and romantic functioning, less engagement in sexual activities, combined with higher sexual anxiety, and higher sexual problems when compared to neurotypical women (Pecora, et. all, 2020). Asexuality, defined as a lack of sexual desire, and objectophilia, a sexual desire for inanimate objects, are more common identities for autistics (Maggio, et. all, 2022). One study estimated that up to 33% of autistic adults appeared to be asexual, but whether this was situational, or a true lack of desire was not determined, asexual identities may be reported due to difficulties in social communication, challenges attaining and maintaining relationships, and sensory challenges associated with autism rather than lack of desire (Gilmour, et. all, 2012). More recent studies found autistic adults have the same sexual desire as neurotypical adults (96% of both have sexual desire) (Maggio, et. all, 2022), and autistics AMAB have been found to engage in sexual activity and have more desire as compared to AFAB autistics (Pecora, et. all, 2016). Autistic lesbian and gay AFAB people are 3.17 times more likely than straight autistic AFAB people to experience unwanted sexual behavior and sexual victimization due to being overly trusting or not picking up on social cues that neurotypical women may perceive more readily as red flags (Pecora, et. all, 2020). Negative sexual experiences may factor into autistic AFAB people identifying more readily with asexual and aromantic identities, as negative sexual experiences can impact a person’s desire or willingness to engage in situations that have previously been harmful. Autism and Sex Differences Contemporary sex definitions are less binary and more malleable than the traditional male/female presented, and youth are more likely to see sex and gender as a spectrum, rather than a binary (Schudson, et. all, 2019). Considering the ability for people to change their biological sex markers through surgery, it is understandable that people are considering sex as a spectrum instead of a static binary. Add to this a growing awareness of intersex identities, including hormonal, chromosomal, or secondary sex characteristic development not matching the sex assigned at birth, and sex identity can become much more complex for autistic people who have a higher rate of androgynous features (Roen, 2019). Research in transgender individuals demonstrates that there may be a biological basis for gender identity that is separate from physical anatomy, such as differences in neuron number and volume in the stria terminalis (Walsh, et. all, 2018). There are a number of physical anomalies associated with autism that may also influence sexuality and gender identity, including brain function differences, biological sex differences, poly-cystic ovarian syndrome (PCOS), and androgen differences (Gasser, et. all, 2022). Biological Sex Differences in Autism Autistic people have a number of atypical physical traits in addition to their neurology that can complicate identity. Their hypothalamus, pituitary, and adrenal glands often function at an impaired rate (Gasser, et. all, 2022). There is an association noted between high birth weight and increased rates of gender non-conformity and autism (Heylens, et. all, 2018) and transgender AFAB autistics have autism profiles more similar to cisgender men than women, which imply causal or correlating factor of gender from autism (Nobili, et. all, 2020). Autistic brains have less connectivity and dimensional variation from typical brain connectivity, but it is not clear whether these patterns develop because of autism or cause autism themselves (Paul, et. all, 2021). Higher autistic traits correlate with higher regional structural brain network efficiency, supporting rigidity of logical thought, routines, and structure common to autism along with difficulty with processing new ideas or conflicting information (Paul, et. all, 2021). Other physical characteristics more common among AFAB autistic adults are more masculine digit ratios, the ring finger being longer than the index finger, and higher facially masculine traits as compared to neurotypical adults (McKenna, et. all, 2021). Conversely, some autistic men demonstrate more feminine facial features and digit ratios, suggesting androgynous features are an indicator of autism in both AMAB and AFAB adults (McKenna, et. all, 2021). Facial masculinity has been found to be predictive of neurodevelopmental conditions and both facial masculinity and masculine digit ratios are associated with impaired social functioning (McKenna, et. all, 2021) Low levels of progesterone are associated with autism and can lead to hirsutism, asexuality, bisexuality, PCOS, irregular menstrual cycle, dysmenorrhea, and higher rates of ovarian, uterine, and prostate cancer in families (Gasser, et. all, 2022). PCOS, the presence of cysts on the ovaries with increased testosterone levels, and delayed menarche are two testosterone linked medical conditions that are present at elevated rates among AFAB autistics (Jones, et. all, 2012). 11.6% of mothers of autistic children had PCOS while they were pregnant, lending credence to male hormone levels in utero increasing the likelihood of autism (Shah & Bobade, 2018). Higher testosterone levels in autistic AFAB people may contribute to associating more with male gender roles (Jones, et. all, 2012). Androgen and Testosterone Pre-Natal Exposure Steroid production, especially androgen hormones are atypical in autistic people, with less progesterone and increased androgen levels, and mothers of autistic people reported low progesterone levels during pregnancy (Gasser, et. all, 2022). Higher rates of male hormones in utero are linked to higher rates of autism diagnosis and higher rates of gender diversity (Heylens, et. all, 2018; McKenna, et. all, 2021). Testosterone affects social connections and higher testosterone levels can mean less interest in socializing (Nobili, et. all, 2020) while lack of progesterone can inhibit a person’s ability to interact well to support well-being of others (Gasser, et. all, 2022). In addition to pre-natal androgen exposure, there are also links between testosterone in adults and autism related traits, including impaired language skills (McKenna, et. all, 2021). The “extreme male brain” theory of autism has been supported in previous studies showing higher androgen exposure rates are associated with increased systematizing tendencies, less typical female gender role presentation, reduced ability to take another person’s perspective (theory of mind), and decreased empathy (Kung, 2020). For some AFAB autistics, increased rates of testosterone lead to an androgynous physical development that can lead to discrimination and harassment, cause confusion about gender identity, or lead to adopting a transgender or non-binary identity (Jones, 2021). Another theory to explain AFAB autistic sexual and gender fluidity is heightened prenatal testosterone often present in autistic pregnancies leading to more masculine traits, presentation, gender identity, and sexuality (Pecora, et. all, 2020). Interestingly, increased pre-natal testosterone is also linked to gay identity development and feminized gender identity for autistic cisgender men (Pecora, et. all, 2020). Discussion for Section Gender non-conformity is prevalent among autistic adults, especially those AFAB, who have higher rates. Transgender people have higher rates of autism than the cisgender population, with transgender men and non-binary AFAB people having the highest rates of autistic traits (Nobili, et. all, 2018). A limitation of many studies is relatively small sample sizes in studies with interviews from one study with 21 individuals (Cooper, et. all, 2022) or 22 individuals (Strang, et. all, 2018), and quantitative studies often having sample sizes of less than 100 transgender individuals (Heylens, et. all, 2018; Kung, 2020; Walsh, et. all, 2018). Many of the research studies looking into gender diversity and autism used the Autism Quotient, a free self-reporting online assessment to determine the degree of autistic traits, which can yield distorted results if respondents mask and change answers to fit expectations or are unsure or ashamed to report their autistic traits (Kung, 2020). There is some contention as to the correlations between autism and gender diversity from a transgender perspective, some theorize that autistic traits such as social anxiety, deficits in communication, and rigid thinking may be mimicked by trauma and that transgender people may simple have elevated autistic traits and not be autistic (Nobili, et. all, 2020). Many studies on the brain function of autistic transgender people could be distorted by elevated rates of anxiety and depression and many of the studies on transgender autistic people viewed transgender identities not as a different and valid way to live but under the gender dysphoria deficit framework that may skew results from research participants who do not feel as comfortable sharing if their words are portrayed in a negative light and may skew interpretation of data collected (Walsh, et. all, 2018). There is also controversy over the extreme male brain theory of autism, some studies have not been able to verify the correlation between pre-natal androgen exposure and increased rates of autism (Kung, 2020; Heylens, et. all, 2018). Digit ratio as a measure of androgen exposure may not be a reliable measure as it is found that digit rations tend to become more feminized with age and inconsistent results are been found, some indicating that most autistic people have masculine digit ratios, and some suggesting that AFAB autistics have masculine and AMAB autistics have feminine digit ratios (McKenna, et. all, 2021). Another concern is that much research on autistic populations was sampled from group homes, which may skew results, as group home residents are more reliant on their caregivers and may internalize the viewpoints of those in authoritative positions (Gilmour, et. all, 2012). An area that research does not well cover is why AFAB autistic people have higher rates of gender and sexuality divergence. An area of need is in researching non-binary identities and autism, much research is still presented using gender binaries and may include transgender men and transgender women,. As autistic people lean more towards the gender spectrum instead of binary gender identities, and may not identify with any gender at all, there is not a strong body of work researching non-binary identities (Ehrensaft, 2018) even though up to 3.9% of the adult population identify as non-binary (Walsh, et. all, 2018). Another area of need in research is in AFAB autistics in general, as most research has relied on the autism diagnosis rates of four males to one female (although rates are estimated to be more accurate at three to one), most research is centered on the male autistic profile and female autistic profiles are underdiagnosed and less understood (Milner, et. all, 2019; Walsh, et. all, 2021).  REFERENCES
Bishop, M. D., Fish, J. N., Hammack, P. L., & Russell, S. T. (2020). Sexual identity development milestones in three generations of sexual minority people: A national probability sample. Developmental psychology, 56(11), 2177–2193. https://doi.org/10.1037/dev0001105 Cooper, K., Mandy, W., Butler, C., & Russell, A. (2022). The lived experience of gender dysphoria in autistic adults: An interpretative phenomenological analysis. Autism, 26(4), 963-974. https://doi-org.csu.idm.oclc.org/10.1177/13623613211039113 Dewinter, J., De Graaf, H., & Begeer, S. (2017). Sexual orientation, gender identity, and romantic relationships in adolescents and adults with Autism spectrum disorder. Journal of Autism & Developmental Disorders, 47(9), 2927–2934. https://doi-org.proxy1.calsouthern.edu/10.1007/s10803-017-3199-9 Ehrensaft, D. (2018). Double Helix Rainbow Kids. Journal of Autism and Developmental Disorders, 48(12), 4079-4081. https://doi-org.csu.idm.oclc.org/10.1007/s10803-018-3716-5 Gasser, B., Kurz, J., Escher, G., Mistry, H. D., & Mohaupt, M. G. (2022). Androgens Tend to Be Higher, but What about Altered Progesterone Metabolites in Boys and Girls with Autism?. Life (Basel, Switzerland), 12(7), 1004. https://doi.org/10.3390/life12071004 Gilmour, L., Schalomon, P. M., & Smith, V. (2012). Sexuality in a community based sample of adults with autism spectrum disorder. Research in Autism Spectrum Disorders, 6(1), 313–318. https://doi.org/10.1016/j.rasd.2011.06.003 Heylens, G., Aspeslagh, L., Dierickx, J., Baetens, K., Van Hoorde, B., De Cuypere, G., & Elaut, E. (2018). The Co-occurrence of Gender Dysphoria and Autism Spectrum Disorder in Adults: An Analysis of Cross-Sectional and Clinical Chart Data. Journal of autism and developmental disorders, 48(6), 2217–2223. https://doi.org/10.1007/s10803-018-3480-6 Janssen, A., Huang, H., & Duncan, C. (2016). Gender Variance Among Youth with Autism Spectrum Disorders: A Retrospective Chart Review. Transgender health, 1(1), 63–68. https://doi.org/10.1089/trgh.2015.0007 Jones, D. B. (2021). De-colonizing my trans body: Fanon and the masks I have worn. Existential Analysis: Journal of the Society for Existential Analysis, 32(2), 322–332. Jones, R. M., Wheelwright, S., Farrell, K., Martin, E., Green, R., Di Ceglie, D., & Baron-Cohen, S. (2012). Brief report: female-to-male transsexual people and autistic traits. Journal of autism and developmental disorders, 42(2), 301–306. https://doi.org/10.1007/s10803-011-1227-8 Kung, K. T. F. (2020). Autistic traits, systematizing, empathizing, and theory of mind in transgender and non-binary adults. Molecular Autism, 11, 1-8. https://doi-org.csu.idm.oclc.org/10.1186/s13229-020-00378-7 Maggio, M. G., Calatozzo, P., Cerasa, A., Pioggia, G., Quartarone, A., & Calabrò, R. S. (2022). Sex and Sexuality in Autism Spectrum Disorders: A Scoping Review on a Neglected but Fundamental Issue. Brain sciences, 12(11), 1427. https://doi.org/10.3390/brainsci12111427 McKenna, B. G., Huang, Y., Vervier, K., Hofammann, D., Cafferata, M., Al-Momani, S., … Michaelson, J. J. (2021). Genetic and morphological estimates of androgen exposure predict social deficits in multiple neurodevelopmental disorder cohorts. Molecular Autism, 12, 1-18. doi:http://dx.doi.org/10.1186/s13229-021-00450-w Milner, V., McIntosh, H., Colvert, E., & Happé, F. (2019). A Qualitative Exploration of the Female Experience of Autism Spectrum Disorder (ASD). Journal of autism and developmental disorders, 49(6), 2389–2402. https://doi.org/10.1007/s10803-019-03906-4 Nobili, A., Glazebrook, C., Bouman, W. P., Baron-Cohen, S., & Arcelus, J. (2020). The stability of autistic traits in transgender adults following cross-sex hormone treatment. International journal of transgender health, 21(4), 431–439. https://doi.org/10.1080/26895269.2020.1783738 Nobili, A., Glazebrook, C., Bouman, W. P., Glidden, D., Baron-Cohen, S., Allison, C., Smith, P., & Arcelus, J. (2018). Autistic Traits in Treatment-Seeking Transgender Adults. Journal of Autism & Developmental Disorders, 48(12), 3984–3994. https://doi-org.csu.idm.oclc.org/10.1007/s10803-018-3557-2 Øien, R. A., Cicchetti, D. V., & Nordahl-Hansen, A. (2018). Gender Dysphoria, Sexuality and Autism Spectrum Disorders: A Systematic Map Review. Journal of autism and developmental disorders, 48(12), 4028–4037. https://doi.org/10.1007/s10803-018-3686-7 Paul, S., Arora, A., Midha, R., Vu, D., Roy, P. K., & Belmonte, M. K. (2021). Autistic traits and individual brain differences: functional network efficiency reflects attentional and social impairments, structural nodal efficiencies index systemising and theory-of-mind skills. Molecular autism, 12(1), 3. https://doi.org/10.1186/s13229-020-00377-8 Pecora, L. A., Hancock, G. I., Hooley, M., Demmer, D. H., Attwood, T., Mesibov, G. B., & Stokes, M. A. (2020). Gender identity, sexual orientation and adverse sexual experiences in autistic females. Molecular autism, 11(1), 57. https://doi.org/10.1186/s13229-020-00363-0 Pecora, L., Mesibov, G., & Stokes, M. (2016). Sexuality in high-functioning autism: A systematic review and meta-analysis. Journal of Autism & Developmental Disorders, 46(11), 3519–3556. https://doi-org.proxy1.calsouthern.edu/10.1007/s10803-016-2892-4 Roen, K. (2019). Intersex or Diverse Sex Development: Critical Review of Psychosocial Health Care Research and Indications for Practice. Journal of Sex Research, 56(4/5), 511–528. https://doi-org.csu.idm.oclc.org/10.1080/00224499.2019.1578331 Schudson, Z. C., Beischel, W. J., & van Anders, S. M. (2019). Individual variation in gender/sex category definitions. Psychology of Sexual Orientation and Gender Diversity, 6(4), 448–460. https://doi.org/10.1037/sgd0000346 Shah, D., Bobade, S. (2018). Polycystic Ovarian Syndrome and Autism. Journal of Psychosocial Research; New Delhi 13(2), 435-442. DOI:10.32381/JPR.2018.13.02.18 Strang, J. F., Powers, M. D., Knauss, M., Sibarium, E., Leibowitz, S. F., Kenworthy, L., Sadikova, E., Wyss, S., Willing, L., Caplan, R., Pervez, N., Nowak, J., Gohari, D., Gomez-Lobo, V., Call, D., & Anthony, L. G. (2018). “They Thought It Was an Obsession”: Trajectories and Perspectives of Autistic Transgender and Gender-Diverse Adolescents. Journal of Autism & Developmental Disorders, 48(12), 4039–4055. https://doi-org.csu.idm.oclc.org/10.1007/s10803-018-3723-6 Subhadip, P., Arora, A., Midha, R., Vu, D., Roy, P. K., & Belmonte, M. K. (2021). Autistic traits and individual brain differences: Functional network efficiency reflects attentional and social impairments, structural nodal efficiencies index systemising and theory-of-mind skills. Molecular Autism, 12, 1-18. doi:http://dx.doi.org/10.1186/s13229-020-00377-8 Varun, W., Greenberg, D. M., Weir, E., Buckingham, C., Smith, P., Meng-Chuan, L., Allison, C., & Baron-Cohen, S. (2020). Elevated rates of autism, other neurodevelopmental and psychiatric diagnoses, and autistic traits in transgender and gender-diverse individuals. Nature Communications, 11(1)https://doi-org.csu.idm.oclc.org/10.1038/s41467-020-17794-1 Walsh, R. J., Krabbendam, L., Dewinter, J., & Begeer, S. (2018). Brief report: gender identity differences in autistic adults: associations with perceptual and socio-cognitive profiles. Journal of Autism & Developmental Disorders, 48(12), 4070–4078. https://doi-org.csu.idm.oclc.org/10.1007/s10803-018-3702-y Warrier, V., Greenberg, D. M., Weir, E., Buckingham, C., Smith, P., Lai, M. C., Allison, C., & Baron-Cohen, S. (2020). Elevated rates of autism, other neurodevelopmental and psychiatric diagnoses, and autistic traits in transgender and gender-diverse individuals. Nature communications, 11(1), 3959. https://doi.org/10.1038/s41467-020-17794-1 GENDER DIVERSITY AND AUTISM: LITERATURE REVIEW OF TRANSGENDER / NON-BINARY AND AUTISM RESEARCH by Lisa Macafee CHAPTER ONE OVERVIEW OF THE STUDY This is a systematic literature review on the relationship of autism and gender diversity, specifically, looking into any heightened gender ambivalence autism produces and correlations in gender diversity, intersex identities, and queer sexualities. Living in the intersecting identities of autistic and queer / transgender results in stigma and marginalization to the individual that may be exacerbated by stigmatizing treatment from mental and physical health care providers who may not well understand the needs of this population (Hall et al., 2020). This cultural competence gap is perpetuated in part by neglecting to include the voices of transgender autistic people in research so causality may be assumed about transgender autistic people by neurotypical cisgender researchers who themselves may not understand their research subjects (Strang et al., 2019). This literature review includes an analysis of previous research looking at autistic people and their understanding and relationships with their gender identity, sex, and sexuality to bring forward perspectives as to causality of the correlation between autism and gender non-conformity and/or queerness (Creswell, 2018). The focus of this literature review is on gender non-conformity in autistic individuals assigned female at birth (AFAB) (Walsh et al., 2018). Autistic women and autistic transgender people are such a small percentage of the population, their intricacies and needs in treatment often go ignored or are lumped in with other similar populations and will benefit from focused attention. Background of the Problem Heightened autistic traits have been found among individuals seeking gender related treatment (up to 35%) and among those who identify as transgender or non-binary (up to 15%) (Kung, 2020; Nobili et al., 2018; Walsh et al., 2018). Of the adult transgender population, 14% are diagnosed as autistic as compared to 0.62% of the general population and 94% of transgender autistics identify as non-binary (Walsh et al., 2018). Walsh et al. (2018) posit autistic individuals reject social conditioning to subscribe to a binary socially imposed gender system when compared to neurotypical peers who may subscribe more to the gender schema and may be more likely to suppress gender incongruence to conform. In one study, 15% of autistic people self-reported a transgender or non-binary identity, with AFAB participants reporting transgender identities 21.6% of the time compared to those assigned male at birth (AMAB) reporting transgender identities 7.8% (Walsh et al., 2018). Highest rates of autistic traits were found among transgender individuals AFAB (45% as compared to 30% for transgender AMAB) (Nobili et al., 2018). Autistic individuals who identify as transgender, non-binary, or gender non-conforming typically experience increased stressors produced from their intersecting identities, primarily difficulties communicating needs around their gender and challenges navigating the complexities of gender expression and identity (Strang et al., 2018). Research on autism and gender diversity done without the voices of those autistic gender-diverse individuals poses problems in data analysis if information is misunderstood or misconstrued (Strang et al., 2019). Attempts to explain the correlation between autism and gender divergence can be harmful to the population if inaccurate or further marginalizing ideas are proposed, for example, some researchers assert autistic transgender individuals may be so only due to sensory difficulties making wearing dresses more preferable for AMAB autistics, which negates their agency and identity as transgender women, attributing their gender identity purely to sensory issues (Maroney & Horne, 2022). It is important to include the voices of those being studied in the research being done for accurate conclusions to be made (Strang et al., 2019). Health care providers have been seeing a higher prevalence of autistic traits among individuals seeking gender affirming care: 14% of those seeking gender affirming care were diagnosed autistic compared to an adult average of 0.62% (Walsh et al., 2018). Autistic individuals are more likely to be transgender for many reasons, one of which being an inherent resistance to social conditioning and expected gender roles allowing for autistic individuals to disregard the binary gender system and reputation management in which many feel the need to comply (Walsh et al., 2018). The most significant correlation of autism and gender was between AFAB autistics identifying as non-binary; only 6% of transgender autistics identified as binary men or women; it seems to be autistic individuals, especially AFAB, are more open to examining their gender identity, less likely to feel pressure to conform to gender norms, and 15% identify as non-binary / transgender compared to 3.9% of the general population (Walsh et al., 2018). There are also elevated autistic traits in transgender people, especially those AFAB, of which; 45% of AFAB transgender people have significantly higher autistic traits than the general population as measured by the Autism Quotient (AQ) as compared to 30% of transgender people AMAB (Nobili et al., 2018). Some research posits transgender people might score higher on the AQ because they often experience more social, health, psychological isolation, pervasive anxiety, and low self-esteem (Nobili et al., 2018). Nobili et al. (2018) posed an “extreme male brain theory” of autism which states, autistic individuals may have been exposed to heightened levels of testosterone in utero causing a drive to systematize, to explain why autism occurs more in men than women (4:1 ratio) and why many AFAB autistics are transgender. Another study showed 15% of transgender men and 19% of AFAB non-binary people meeting autism cut-offs rates while those AMAB did not meet significant cut-offs for autism leading researchers to theorize autistics may have more of a testosterone-influenced brain influencing those AFAB to present more masculine (Kung, 2020). Autism is more common among transgender individuals; about 15% of autistic individuals identify as transgender, non-binary, or gender non-conforming, much higher than the general transgender rates in the population (Maroney & Horne, 2022). Autistic transgender people experience intersectional stigmas of ableism and cissexism including barriers to accessing health care, discrimination, and access challenges (Maroney & Horne, 2022); 58.2% of therapists said they know about examples of bias in treatment from their peers towards the queer community, only 34% of psychology graduates reported diversity education as part of their training, and LGBTQ+ clients have reported perceptions of heterosexism from therapists and dissatisfaction with their treatment (Carroll & Gilroy, 2001). Autistic people AFAB are 1.68 times more likely to be transgender, 2.39 times more likely to be gay, and 2.33 times more likely to be bisexual when compared to non-autistic women (Pecora, 2020). Autistic gay women reported experiencing regrettable sexual experiences 2.72 times as often and unwanted sexual behaviors 3.17 times as often as autistic heterosexual women while autistic women overall experienced unwanted sexual experiences 2.98 times more than non-autistic women (Pecora, 2020). It is important for mental and physical health care practitioners to have accurate information on marginalized populations to be able to best support them. It is estimated autistic AFAB people have these higher rates of adverse sexual experiences partially due to the higher rates of sexual victimization among gender diverse populations, as transgender women reported regrettable sexual experiences 4.01 times more often than cisgender women, and other causes of aversive experiences are linked to autistic people’s lessened ability to perceive red flags due to social impairment in relationships or communicate needs as well as non-autistic people (Pecora, 2020). Add to this the additional struggle women are often missed in diagnosis for autism, it is estimated the true ratio of autism in men to women is 3:1 and not 4:1 as the rate diagnosed because many diagnosing practitioners are not adept at diagnosing women; (Zener, 2019). Autistic women diagnosed after age 18 are more likely to be diagnosed with PTSD (up to 17% of autistic women) due to trauma exposure, depression, and misdiagnosis, more have eating disorders (up to 30% of women with anorexia qualify for an autism diagnosis), and many struggle with diagnosis of borderline personality disorder, obsessive compulsive disorder, burnout, or failure to launch challenges (Zener, 2019). For many neurodivergent people, their identities are already seen as “queer” by mainstream society, as disability has been pathologized by medicine and religion as other and less than, which have systemic impacts on the transgender autistic community (Abrams & Abes, 2021). According to Hall et al. (2020), LGBTQ+ autistic people experience more than double the rates of mental health concerns (78.9% versus 34.3%) and days of bad physical health per month (11.1 versus 5.1). They smoked almost ten times more (26.3% versus 2.9%), had higher unmet health care needs (73.7% versus 43.8%), and had been refused health care more (35.7% versus 20%) when compared to their cisgender/straight autistic peers (Hall et al., 2020). Transgender people experience heightened levels of mental health problems, notably in anxiety, depression, and self-harm; higher levels of autistic traits among transgender people may be due to chronic stress manifesting as autistic traits (Nobili et al., 2018). Autistic gender diverse individuals are especially likely to struggle with finding and receiving appropriate health care, navigating relationships, and assess safety concerns while also trying to create affirming community due to stigma and negative experiences experienced causing hesitancy to self-advocate (Maroney & Horne, 2022). Problem Statement The problem being investigated is the lack of cultural competence among mental health care providers for queer autistic people causing missed or misdiagnosis and results in inappropriate treatment causing harm to gender diverse autistic people (Hall et al., 2020). The DSM-V defines autism strictly as the absence of neurotypicality instead of neutral statements of what is autism (Maroney & Horne, 2022). Health disparities exist for autistic individuals who are also LGBTQ+ (Hall et al., 2020). Misunderstanding populations or misattributing traits to them they do not identify with can cause populations harm, with decreased mental and physical health outcomes, and yet, few voices of autistic people are involved in research to help explain these concerns (Strang et al., 2019). It is important accurate and recent research is used to determine best practices, including voices from autistic gender diverse people themselves to explain the issues as they see them, to prevent assumptions of causality based on neurotypical perspectives contributing to the existing mental health disparities (Maroney & Horne, 2022). Purpose of the Study The purpose of this systematic literature review is to provide a cohesive body of knowledge summarizing recent research on transgender/non-binary and autistic treatment, correlations, and issues. This literature review includes analysis of recent research to identify how transgender and non-binary autistic people perceive gender and sexuality, how they see gender and sexuality relating to autistic traits they have, and treatment recommendations and best practices. This review includes summaries of research in a comprehensive, culturally sensitive, and inclusive manner. Research studies will be examined from ProQuest, EBSCOHost, Google Scholar, and PsychiatryToday databases, along with some excerpts from books and grey articles. Research Questions RQ1. What does research data demonstrate as to the relationship between autistic adults (especially those AFAB) and non-binary and transgender identities? RQ2. How do autistic adults’ sex, gender, and gender identity differences develop? RQ3. What mental health treatment methods and practices are recommended to best serve the transgender and non-binary autistic population? Theoretical Framework Autism and gender identity will be analyzed through the theoretical lenses of queer theory and crip theory. These theories help frame the problem of autistic transgender people being ill-treated due to ignorance, bias, or lack of understanding in the research on autistic transgender people (Creswell, 2018). Queer theory is founded in questioning the norms of gender and sexuality enforced by society (Carroll & Gilroy, 2001). This is especially pertinent for queer autistic people as they may not intuit the roles others expect them to take and may have less ability to identify barriers due to sexuality or gender identity and how to address them due to their autistic nature. For many, sex, gender, and sexuality are performative acts based on the internalization of societal expectations and the individual’s situation and sexual orientation and gender identity change over time and are not pre-determined (Verma et al., 2023). Queer theory resists normalizing and privileging certain identities over others and encourages society to resist policing other people’s expressions outside of the commonly accepted binary identities (Verma et al., 2023). People do not all fit conveniently into the gender binaries presented (male/female) and queer theory helps to break down some of the heteronormative structures and pressure to conform, question assumptions about gender and sexuality, focus on the systems of power that divide, and support people who identify as transgender or non-binary (Carroll & Gilroy, 2001). According to Jones (2021), transgender people are often given more privilege and power in society if they perform a cisgender role, but this may feel inauthentic to their true self and prevent them having genuine relationships for fear of being “found out”. Conversely, adopting a queer identity as a transgender person risks danger and abuse in the world; attaining a state of good mental health may be very difficult for some without the rejection of the binary and safe living situations (Jones, 2021). Queer theory posits by not adhering to gender binaries, queer and transgender people disrupt systems of power contributing to others living artificially or stigmatizing roles due to fear and allowing others to question their assumptions on gender and sexuality (Jones, 2021). Queer theory has been a political rallying cry to encourage individuals to think outside the hegemonic boxes society has construed as the only options and has encouraged people to create new ways of being that do not involve being stuck inside of binary socially prescribed attitudes and beliefs (Burns, 2021). It is important when individuals realize the roles they have internalized to perform become restrictive or harmful, they develop a cultural flexibility allowing them to leave paradigms not serving them behind to forge a better future for themselves (Kokkos, 2022). Queer theory emphasizes the importance of critically evaluating schemas purported to be “normal” (such as gender roles) to identify harmful elements perpetuated in order to keep certain populations in power and others minoritized (Kokkos, 2022). Similarly, crip theory, created by Robert McRuer in the early 2000s, was made to deconstruct ideas about disability and being disabled and focuses on how reality can be re-shaped and re-imagined to allow for other ways of being to exist in the world and avoids use of the word “normal” in favor of modalities allowing individuals to, not just survive, but flourish, while existing outside of assimilation and typicality (Kafer, 2009). Crip theory rejects ableism (compulsory able-mindedness and able-bodiedness); ableism states bodies and minds more typical are therefore more valuable, and bodies and minds veering further from “normal” are therefore less deserving of space in the world; but disability is a naturally occurring variation in humans and all people are normal – although all people are not typical (Abrams & Abes, 2021). For people who are disabled and queer, assimilationist ideologies will never work to build authentic paradigms of power and privilege, because the individual will always be fundamentally different from what is expected as typical. Essentially, crip theory argues while queer disabled people are constantly being displaced by society, the brightest possibilities come about in the refusal of displacement (Kafer, 2009). Just as the word queer encompasses a variety of identities under the LGBTQ+ umbrella, the word disability also encompasses spectrums of differences and society has seemingly deemed both groups inferior to the able-bodied, neurotypical, cisgender, heterosexual person, which causes people in marginalized identities challenges (Kafer, 2009). Autism is associated with higher rates of transgender identities and these two intersecting marginalized identities produce stigma to the individuals who live in this intersection and part of this marginalization is brought on by a biased and stigmatizing view of mental and physical health care providers who do not well understand the needs of this population (Hall et al., 2020). This is perpetuated in part by neglecting to include the voices of transgender autistic people in research and causality is often assumed about this population by neurotypical cisgender researchers who themselves may not understand this population (Strang et. al., 2019). This literature review includes an exploration of the correlation between autism and gender non-conformity utilizing queer theory and crip theory as frameworks for alternate ways people may exist and be empowered in the world and to guide the line of inquiry away from reinforcing societal norms to attempt an honest exploration of the issues at hand (Creswell, 2018). Definitions and Key Terms Assigned Female at Birth (AFAB) Transgender people who were assigned female at birth (AFAB) are often referred to as AFAB to denote which gender they were assigned before or irrespective of transition, a transgender man was typically AFAB (Nobili et al., 2018). Assigned Male at Birth (AMAB) Transgender people who were assigned male at birth (AMAB) are often referred to as AMAB to denote which gender they were assigned before or irrespective of transition, a transgender woman was typically AMAB (Nobili et al., 2018). Autism or Autistic Autism is a fundamental difference in the way people interact and communicate that includes differences in thinking, socialization, sensory processing, and communication and at times, autism is referenced to under the umbrella term of neurodiversity, which includes other neuro-minorities (Maroney, Horne, 2022). Throughout this paper, both “individual with autism” and “autistic individual” are used interchangeably. As a note, the autism community generally prefers identity-first language (autistic person) while the disability rights community as a whole generally prefers person-first language (person with autism) (Carroll, 2019). Cisgender Cisgender described people whose gender identity matched what they were assigned at birth, for example a cisgender woman was assigned female at birth and identifies as female as an adult (Nobili et al., 2018). Intersex To be intersex means an individual has had a natural diverse sexual development outside of the typical male/female binary in physical sex characteristics, hormones, or chromosomes (Roen, 2019). Queer Queer is an umbrella term including nonnormative sexualities such as gay, bisexual, and pansexual as well as nonnormative gender identities such as transgender, non-binary, and gender fluid, among many others; queer is a way to identify many minoritized groups under one identity (Burns, 2021). Non-Binary / Transgender / Gender Diverse / Gender Non-Conforming Transgender is used as an umbrella term in this paper and is used to describe anyone who do not identify 100% with the gender assigned to them at birth, including transgender binary identities (transgender men and transgender women), transgender non-binary identities such as (non-binary, agender), gender diverse identities (such as third gender, gender fluid, bi-gender), and gender non-conforming individuals (Strang et al., 2019). 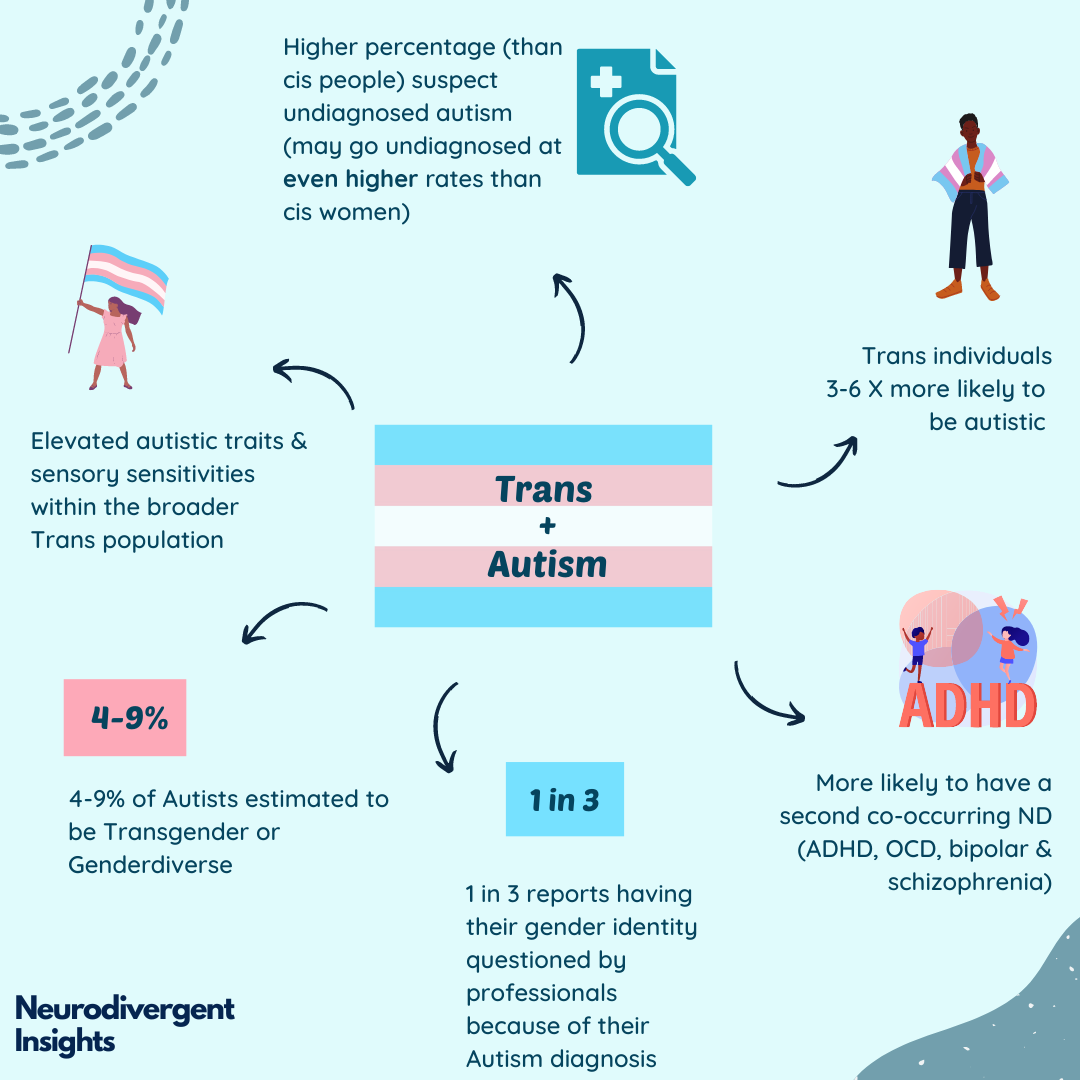 REFERENCES
Abrams, E. J., & Abes, E. S. (2021). "It's Finding Peace in My Body": Crip Theory to Understand Authenticity for a Queer, Disabled College Student. Journal of College Student Development, 62(3), 261-275. http://proxy1.calsouthern.edu/login?url=https://www-proquest-com.csu.idm.oclc.org/scholarly-journals/finding-peace-my-body-crip-theory-understand/docview/2547639324/se-2 American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, DSM-5. American Psychiatric Association Publishing. Burns, R. (2021). Queerness as/and political attunement: a brief response to Anderson & Knee (2020) Queer Isolation or Queering Isolation? Leisure Sciences, 43(1/2), 125–130. https://doi-org.csu.idm.oclc.org/10.1080/01490400.2021.1874575 Carroll, L., & Gilroy, P. J. (2001). Teaching “Outside the Box”: Incorporating Queer Theory in Counselor Education. Journal of Humanistic Counseling, Education & Development, 40(1), 49–58. https://doi-org.csu.idm.oclc.org/10.1002/j.2164-490X.2001.tb00101.x Carroll, S. (2019). Respecting and empowering vulnerable populations: Contemporary terminology. The Journal for Nurse Practitioners, 15(3), 228-231. https://doi-org.csu.idm.oclc.org/10.1016/j.nurpra.2018.12.031 Creswell, J. W. (2018). Research design: Qualitative, quantitative, and mixed methods approaches. (5th ed.). Sage. Hall, J. P., Katie, B., Streed,Carl G.,,Jr, Boyd, B. A., & Kurth, N. K. (2020). Health disparities among sexual and gender minorities with autism spectrum disorder. Journal of Autism and Developmental Disorders, 50(8), 3071-3077. https://doi-org.csu.idm.oclc.org/10.1007/s10803-020-04399-2 Jones, D. B. (2021). De-colonizing my trans body: Fanon and the masks I have worn. Existential Analysis: Journal of the Society for Existential Analysis, 32(2), 322–332. Kafer, A. (2009). What's Crip About Queer Theory Now?: Crip Theory: Cultural Signs of Queerness and Disability. By Robert McRuer, New York, New York University Press, 2006. 283 pp. $22.00 (paperback). ISBN-10: 0814757138. Sex Roles, 60(3-4), 291-294. https://doi-org.csu.idm.oclc.org/10.1007/s11199-008-9511-6 Kokkos, A. (2022). Transformation theory as a framework for understanding transformative learning. Adult Education – Critical Issues (2)2, 20-33. Retrieved from https://www.researchgate.net/publication/366826194_Transformation_Theory_as_a_Framework_for_Understanding_Transformative_Learning on May 31st 2023. Kung, K. T. F. (2020). Autistic traits, systematizing, empathizing, and theory of mind in transgender and non-binary adults. Molecular Autism, 11, 1-8. https://doi-org.csu.idm.oclc.org/10.1186/s13229-020-00378-7 Maroney, M. R., & Horne, S. G. (2022). “Tuned into a different channel”: Autistic transgender adults’ experiences of intersectional stigma. Journal of Counseling Psychology, 69(6), 761–774. https://doi-org.csu.idm.oclc.org/10.1037/cou0000639.supp (Supplemental) MasterClass. (2022). Queer Theory: Definition, history, and impact. Retrieved from https://www.masterclass.com/articles/queer-theory on May 31st, 2023. Nobili, A., Glazebrook, C., Bouman, W. P., Glidden, D., Baron-Cohen, S., Allison, C., Smith, P., & Arcelus, J. (2018). Autistic Traits in Treatment-Seeking Transgender Adults. Journal of Autism & Developmental Disorders, 48(12), 3984–3994. https://doi-org.csu.idm.oclc.org/10.1007/s10803-018-3557-2 Pecora, L. A., Hancock, G. I., Hooley, M., Demmer, D. H., Attwood, T., Mesibov, G. B., & Stokes, M. A. (2020). Gender identity, sexual orientation and adverse sexual experiences in autistic females. Molecular Autism, 11, 1-16. https://doi-org.csu.idm.oclc.org/10.1186/s13229-020-00363-0 Roen, K. (2019). Intersex or Diverse Sex Development: Critical Review of Psychosocial Health Care Research and Indications for Practice. Journal of Sex Research, 56(4/5), 511–528. https://doi-org.csu.idm.oclc.org/10.1080/00224499.2019.1578331 Strang, J. F., Klomp, S. E., Caplan, R., Griffin, A. D., Anthony, L. G., Harris, M. C., Graham, E. K., Knauss, M., & van der Miesen, A. I. R. (2019). Community-based participatory design for research that impacts the lives of transgender and/or gender-diverse autistic and/or neurodiverse people. Clinical Practice in Pediatric Psychology, 7(4), 396–404. https://doi-org.csu.idm.oclc.org/10.1037/cpp0000310 Strang, J. F., Powers, M. D., Knauss, M., Sibarium, E., Leibowitz, S. F., Kenworthy, L., Sadikova, E., Wyss, S., Willing, L., Caplan, R., Pervez, N., Nowak, J., Gohari, D., Gomez-Lobo, V., Call, D., & Anthony, L. G. (2018). “They Thought It Was an Obsession”: Trajectories and Perspectives of Autistic Transgender and Gender-Diverse Adolescents. Journal of Autism & Developmental Disorders, 48(12), 4039–4055. https://doi-org.csu.idm.oclc.org/10.1007/s10803-018-3723-6 Verma, T., Chapman-Orr, E., Davis, A. What is queer theory? Grinnell College: Subcultures and Society. Retrieved from https://haenfler.sites.grinnell.edu/subcultural-theory-and-theorists/queer-theory/ on May 31st, 2023. Walsh, R. J., Krabbendam, L., Dewinter, J., & Begeer, S. (2018). Brief report: gender identity differences in autistic adults: associations with perceptual and socio-cognitive profiles. Journal of Autism & Developmental Disorders, 48(12), 4070–4078. https://doi-org.csu.idm.oclc.org/10.1007/s10803-018-3702-y Zener, D. (2019). Journey to diagnosis for women with autism. Advances in Autism, 5(1), 2-13. https://doi-org.csu.idm.oclc.org/10.1108/AIA-10-2018-0041 Considerations in Autism Support Consultation |
Hello friends! I would like to publish writings from myself and other people with autism as snapshots of how autism has affected them, since there are so many misconceptions and confusions about adults with autism.
Some background: I completed a 12 unit certificate program to be able to serve autistic students and am angry at how the program focused only on little boys as autistic and completely left out adults, the trans autistic population, and girls/ femmes/ women autistics. I am currently pursuing a PsyD to do more research on autism and gender. Please contact me if you would like to add a story! If so, please send me your piece, publish name, title, and an image (can be a picture related to your content, your picture, an autism meme, etc). I am interested in publishing this collection, because people don't know enough about us (but sure do assume a lot). Also on Facebook! AuthorLisa Macafee, autistic counselor with a hankering for social justice. Archives
March 2024
Categories |

 RSS Feed
RSS Feed